Case History
A 55-year-old female with a pelvic mass, laterality unknown; surgeon favors that the mass involves both adnexa and not sure which side it originated from. On gross examination there is a 17-cm complex, multilocular cyst with notable foci that show cystic, solid and papillary structures.
- What is the most appropriate diagnosis?
- High-grade serous carcinoma with clear cell change
- Renal cell carcinoma
- Yolk sac tumor
- Clear cell carcinoma of the ovary
- What entity is commonly associated with this lesion?
- Endometriosis
- Endosalpingiosis
- Endocervicosis
- Paratubal cysts
- These tumors can present with …
- Abdominal pain and swelling
- Symptoms related to endometriosis
- Asymptomatic
- All of the above
Answers:
1. d. Clear cell carcinoma of the ovary
2. a. Endometriosis
3. d. All of the above
Discussion:
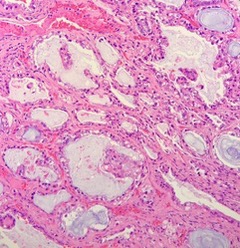
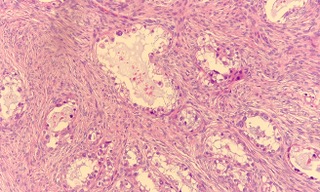
Clear cell carcinoma (CCC) of the ovary are rare malignant carcinomas which comprise ~5-10% of all surface epithelial carcinomas. The typical presentation is in a peri- to postmenopausal woman. CCC usually presents with abdominal pain, swelling, symptoms related to endometriosis, and may be associated with a paraneoplastic syndrome or, in some cases, no symptoms at all.
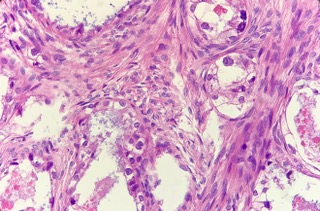
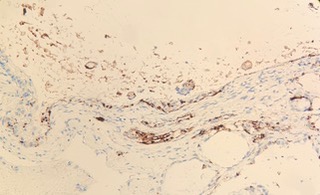
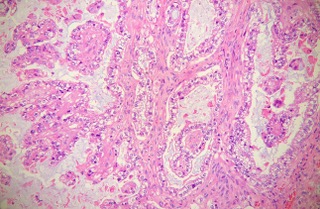
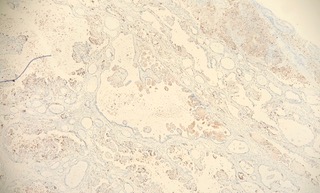
CCCs comprise 10% of endometriosis-related carcinomas and are associated with ARID1A and PIK3CA mutations. CCC are mostly unilateral, cystic and can have a solid component. Necrosis and hemorrhage are common. Tubulo-cystic and papillary architectures are most common. Mucin/colloid can be seen in the lumen. Cytologically, one can sees hobnail cells with nuclear hyperchromasia and clear to granular cytoplasm. There is often marked nuclear atypia and prominent nucleoli. These cells line tubules and cystic structures. Immunohistochemically, CCCs are positive for CK7, EMA, PAX8, NapsinA. ER/PR variable/negative and WT1,SALL4 are negative. P53 shows wild-type expression.
Stage 1C (rupture or + washings) associated with worse prognosis.
Case contributed by Dina Kokh, M.D., Assistant Professor, Anatomic Pathology, UAB Department of Pathology