Case History
A 60-year-old woman presented with a small, irregular breast mass on imaging. A biopsy was performed.
- Invasive ductal carcinoma, grade 1
- Invasive tubular carcinoma, grade 1
- Radial scar
- Sclerosing adenosis
Answer:
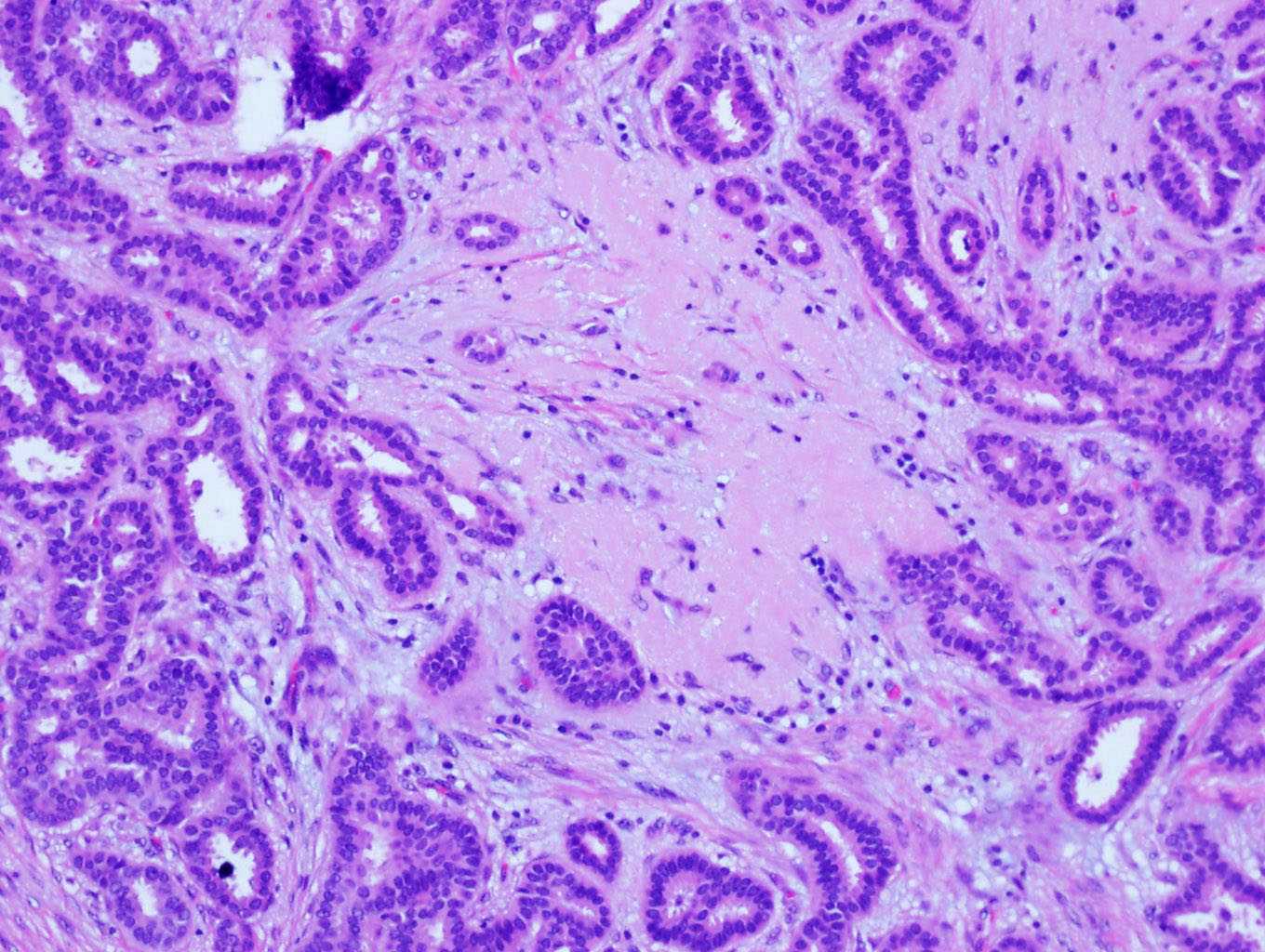
The answer is “B”, invasive tubular carcinoma.
Discussion: The characteristic histologic features of tubular carcinoma are well-formed glands or tubules arranged in haphazardly arranged, infiltrative growth pattern. The glands/tubules are composed of a single layer of epithelial cells enclosing an open lumen. The surrounding myoepithelium is absent. The neoplastic glands are typically a mixture of oval, rounded, and angulated contours with tapering ends. There is no universal agreement for the cutoff regarding the proportion of tubular structures required for a diagnosis of tubular carcinoma. It is recommended by WHO Classification that these structures should comprise >90% of the lesion for a tumor to be categorized as a “pure” tubular carcinoma, and those with 50-90% tubular elements should be regarded as being of mixed type. The cells are small to intermediate in size with grade 1 or 2 nuclei and often exhibit apical snouts. Calcifications may be associated with secretory materials in lumens. Nuclear stratification, significant nuclear pleomorphism and high mitotic index are contraindications for a diagnosis of tubular carcinoma. It is important to recognize tubular carcinoma as the patients with this special type of breast cancer have an excellent prognostic outcome when compared to invasive carcinoma no special type (invasive ductal carcinoma).
Another important feature of tubular carcinoma is the prominent desmoplastic stromal reaction. Stromal elastosis may be present in some cases. A spectrum of low grade lesions are commonly seen in association with tubular carcinoma, including flat epithelial atypia, low grade DCIS and, less frequently, lobular neoplasia. The combination of tubular carcinoma, columnar cell lesions, and LCIS is known as “Rosen Triad”.
References
- Rakha E, Pinder SE, Shin SJ, Tsuda H. Tubular carcinoma and cribriform carcinoma. In: Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, eds. WHO Classification of Tumours of the Breast. Lyon: IARC Press; 2012:43-5.
- Tubular carcinoma and cribriform carcinoma. In: Hameed O, Wei S, Desouki MM, Humphrey H, eds. Advances in Surgical Pathology: Breast Cancer. Philadelphia: LWW; 2015:72-80.
Case contributed by Shi Wei, M.D., Ph.D., Professor, Anatomic Pathology, UAB Department of Pathology