Case History
A 35-year-old with a unilateral pelvic mass.
What is the likely diagnosis?
- Endometrioid carcinoma
- Carcinoid tumor
- Sertoli–Leydig cell tumor
- Metastatic carcinoma
- Granulosa cell tumor
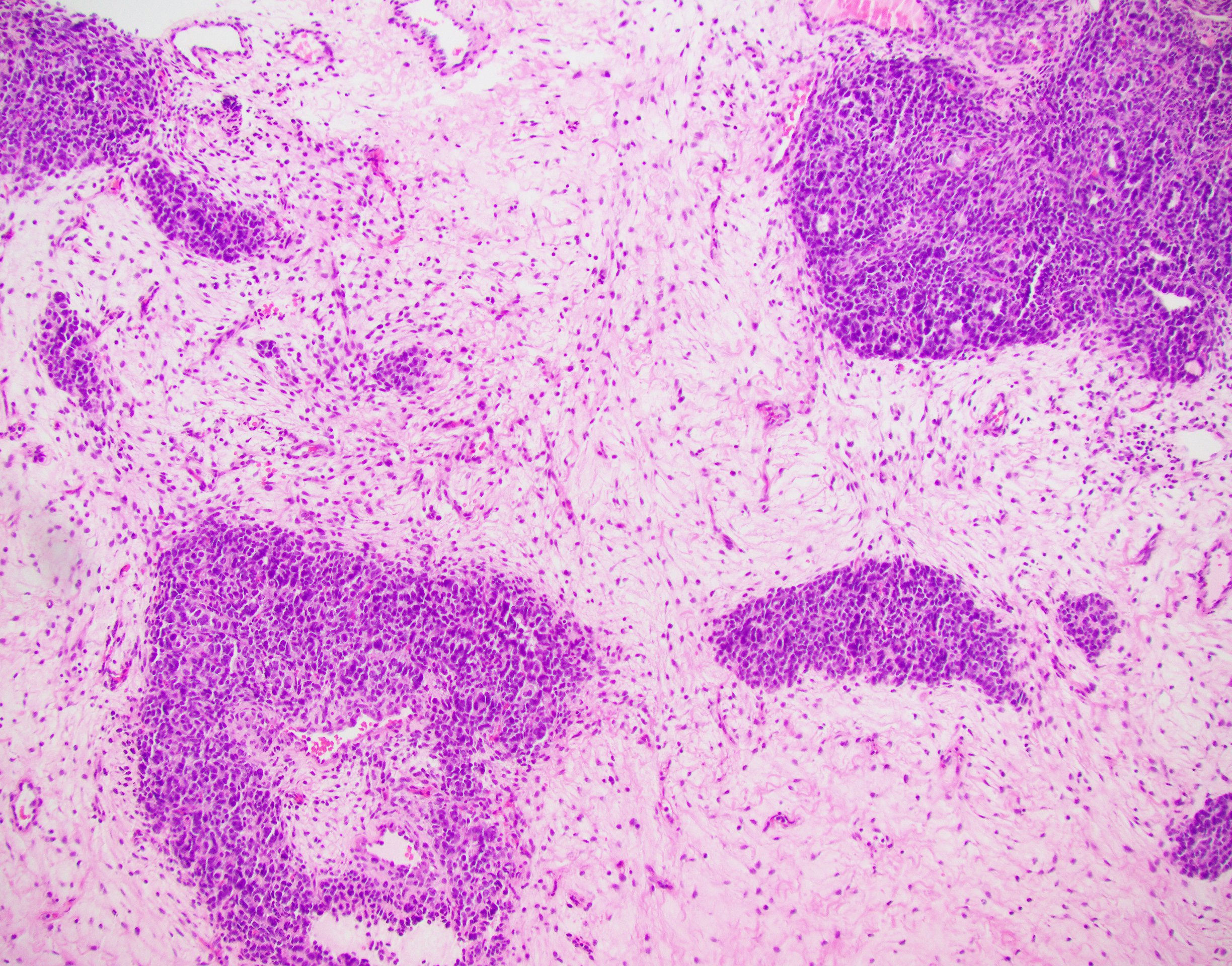
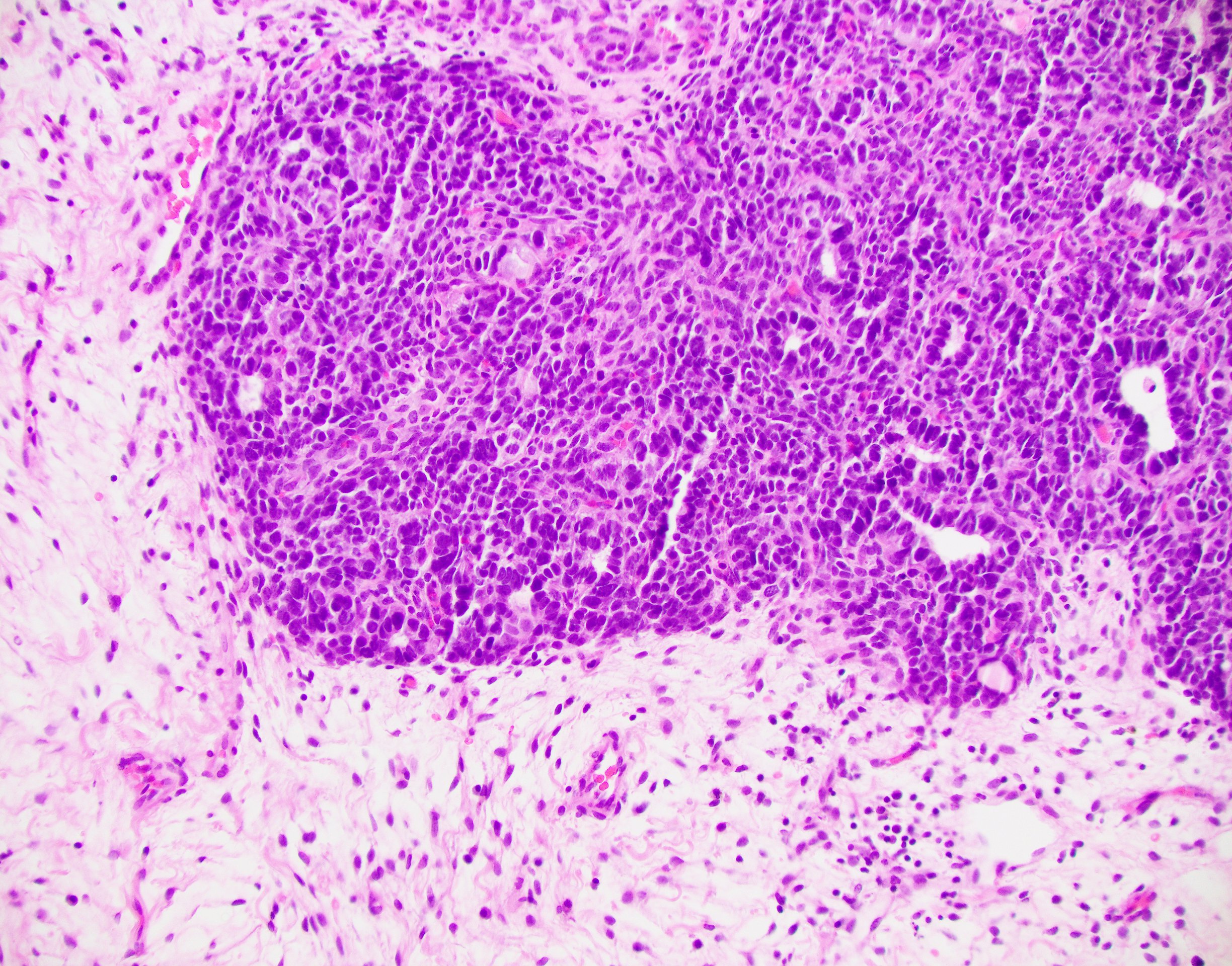
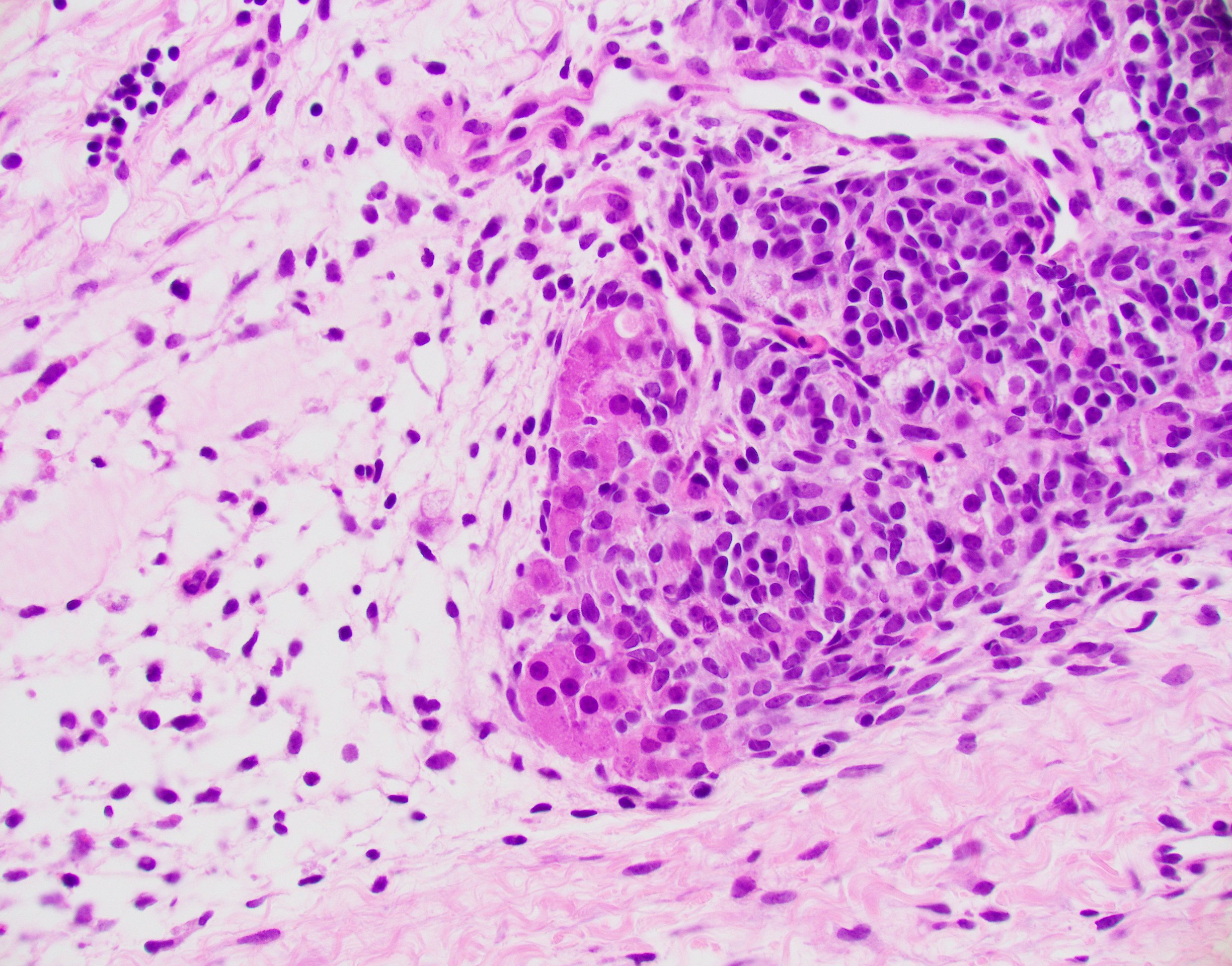
Answer: This tumor shows hypercellular and hypocellular areas. The hypercellular areas consist of clusters of darkly staining ovoid to spindle cells with scant cytoplasm with focal tubular differentiation intermixed with scattered nests of uniform cells with small round nuclei and abundant eosinophilic cytoplasm. The nuclei are not cleaved and sarcomatoid areas are not identified. All these histologic features are suggestive of Sertoli–Leydig cell tumor, moderately differentiated. Immunohistochemically, the tumor cells are positive for inhibin, calretinin, SF-1, and negative for EMA and CK7, supporting the diagnosis of Sertoli-Leydig cell tumor. Endometrioid carcinomas are positive for CK7 and EMA. Leydig cells are not present in fibrothecoma and granulosa cell tumor. Granulosa cell tumor typically shows cleaved (coffee bean like) nuclei.
Sertoli–Leydig cell tumors are rare, typically occurring in young women, and usually unilateral. It may show androgenic or rarely estrogenic manifestations. These tumors are graded as follows: well differentiated, moderately differentiated, and poorly differentiated. Recently, Sertoli-Leydig cell tumors are described to have DICER-1 mutation, which may be germline or sporadic. Sertoli-Leydig cell tumor may have heterologous elements or reticular pattern. Histologic grade and subtyping correlates with the clinical behavior.