Case History
The patient is a 30-year-old female with a 2.5 cm left upper pole renal mass
What is the diagnosis?
- Chromophobe renal cell carcinoma
- Succinate dehydrogenase (SDH)-deficient renal cell carcinoma
- Fumarate hydratase (FH)-deficient renal cell carcinoma
- Translocation-associated renal cell carcinoma
Answer: D. Translocation-associated renal cell carcinoma
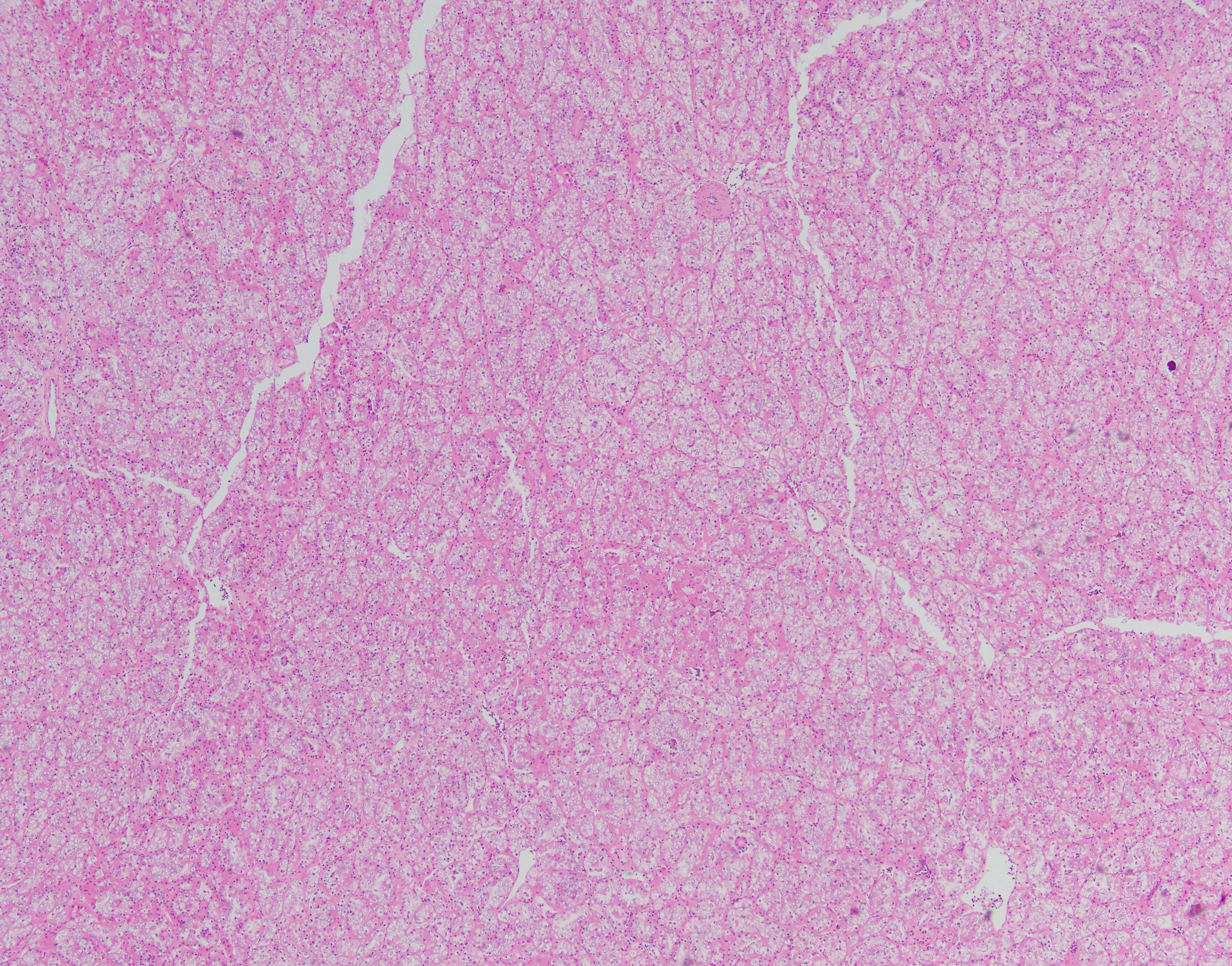
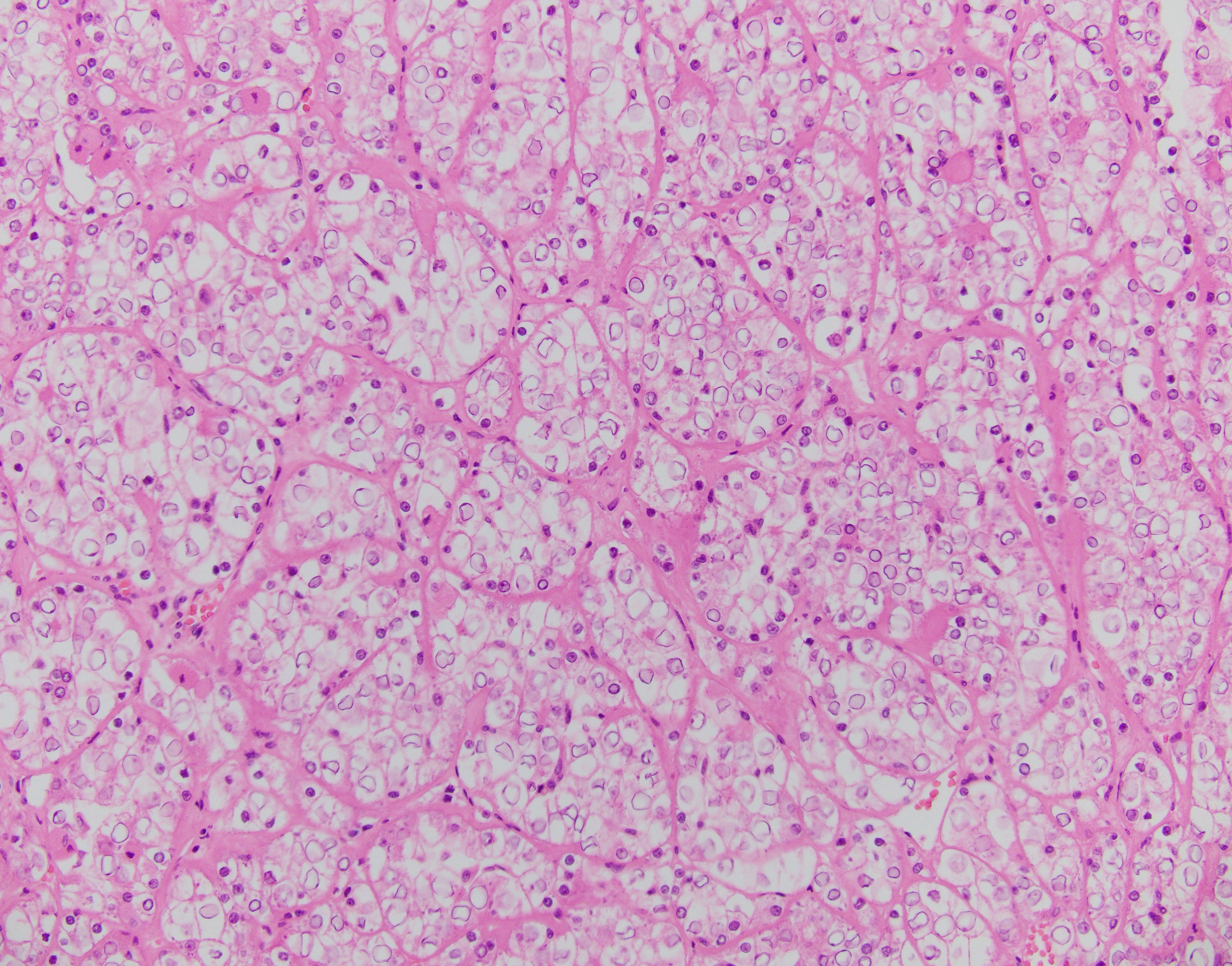
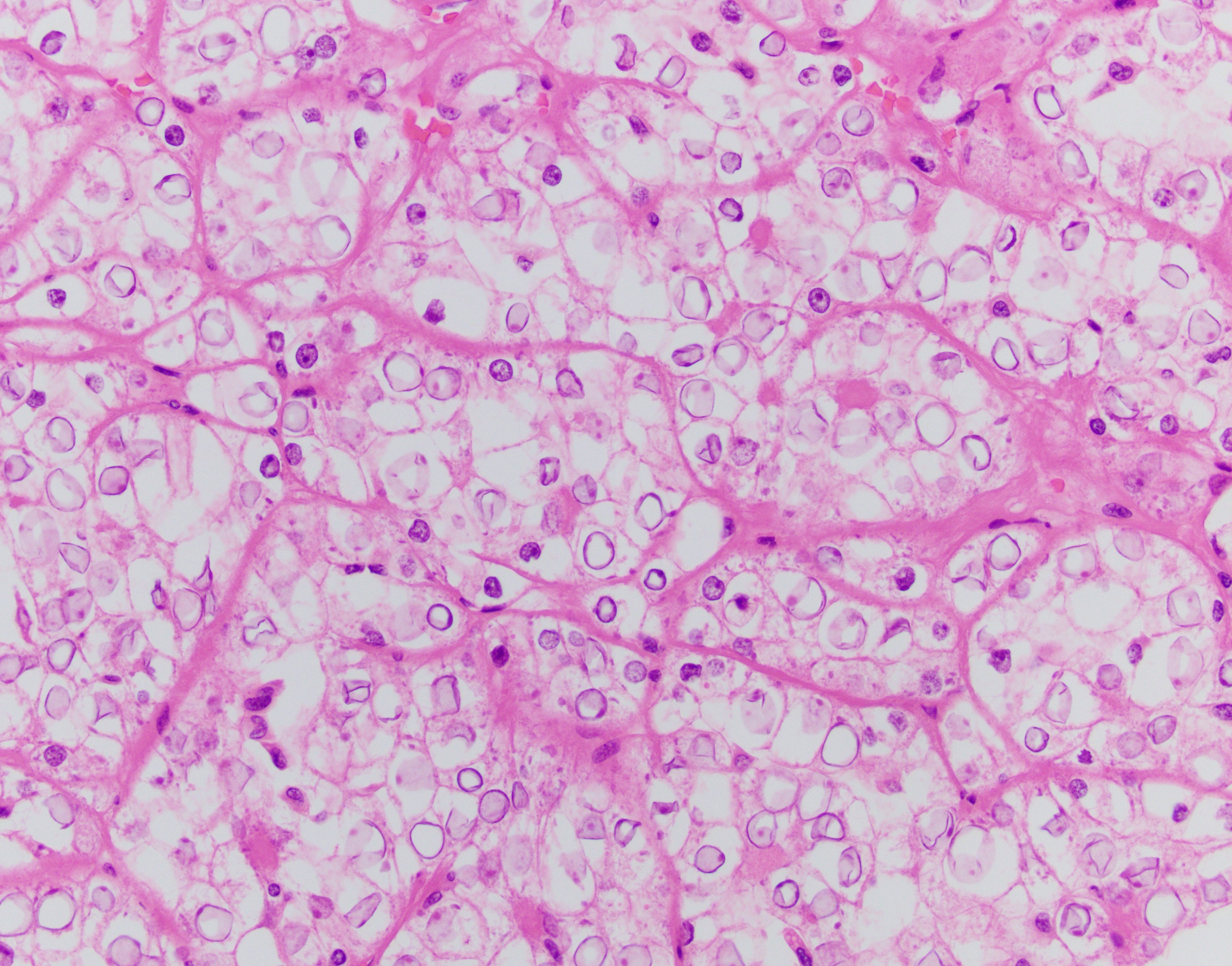
The neoplasm has a compact architectural growth pattern with confluent anastomosing cords, tubules and acini. The tumor cells have granular eosinophilic cytoplasm containing glycogen. The nuclei are round to oval with slightly irregular contours, having a distinct chromatin pattern with condensation at the periphery with clearing of the central portion.
The tumor cells are positive for cathepsin K and Pax8. FH is retained. CA-9 is negative. SDHB is retained and 2-succinocysteine (2SC) is negative, and PAS highlights intracytoplasmic glycogen. In the context of the morphologic features, these adjunctive immunohistochemical findings support the diagnosis renal cell carcinoma, although the pattern of staining is not entirely specific.
The positive staining for cathepsin K raises the possibility of a translocation-associated renal cell carcinoma, so FISH for TFE3 and TFEB was performed at Mayo Clinic Laboratories. Tumor cells showed rearrangement of the TFEB locus. Rearrangement of the TFEB gene at 6p21.1 is associated with t(6;11) renal cell carcinoma. The main translocation partner gene is MALAT1 at 11q12.
Translocation-associated RCCs involve the MiTF/TFE (Microphthalmia-associated transcription factor/transcription factor binding to IGHM enhancer 3) family genes. The primary genes involved are either TFE3 (located at Xp11.2) or TFEB (located at 6p21.1). Due to the relatively small number of cases studied so far, knowledge of the clinical aspects and outcome of these tumors is not complete. They do represent at least 20% of RCCs in the pediatric age group. Histologically, t(6;11) carcinomas usually consist of nests and microscopic cysts composed of polygonal cells with pale or eosinophilic cytoplasm. Papillae are uncommon. These cells can be arranged around nodules of hyaline material in large acini.