Case History
84-year-old female with 1.5 cm right breast mass, s/p lumpectomy. The tumor is diffusely and strongly positive for CK7 and Cam 5.2, weakly positive for GATA3, and negative for Calponin. CK5/6, smooth muscle myosin, S100, smooth muscle actin show variable positivity. ER, PR, HER2 and AR are negative. TRSP1 is positive. Ki67 is 10%.
What is the most likely diagnosis?
B. Invasive ductal carcinoma
C. Epithelial-Myoepithelial carcinoma
D. Adenoid cystic carcinoma
Answer: C. Epithelial-Myoepithelial carcinoma
Neoplastic biphasic epithelial–myoepithelial lesions of the breast include adenomyoepithelioma (AME), pleomorphic adenoma and adenoid cystic carcinoma. AME can be benign or malignant.
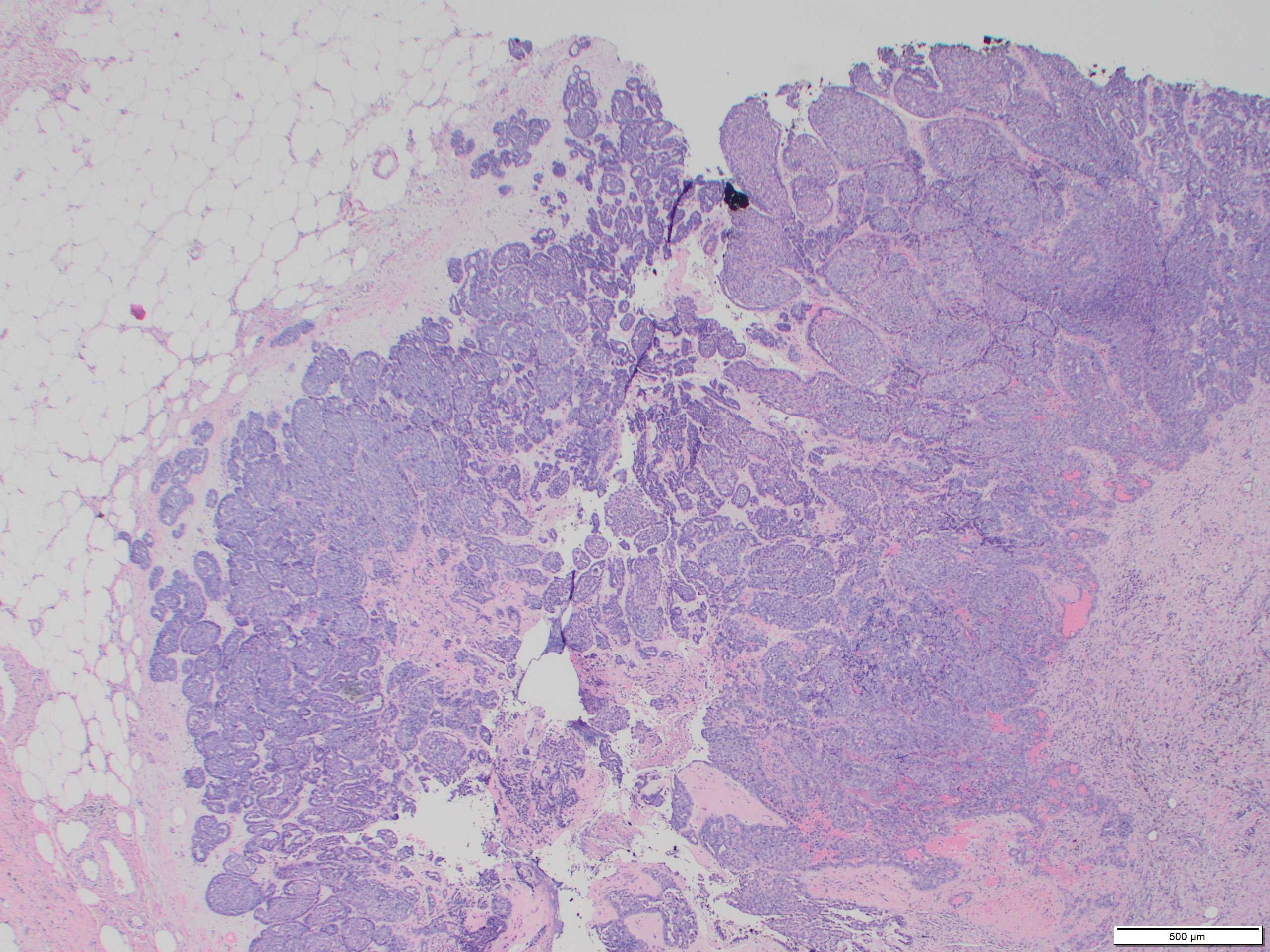
Classic AME is rare, accounting for less than 0.5% of breast tumours. It predominantly affects older women. Radiologically, AME forms a round or lobulated dense mass with margins that may be indistinct. Local recurrences have been reported in approximately 10%.
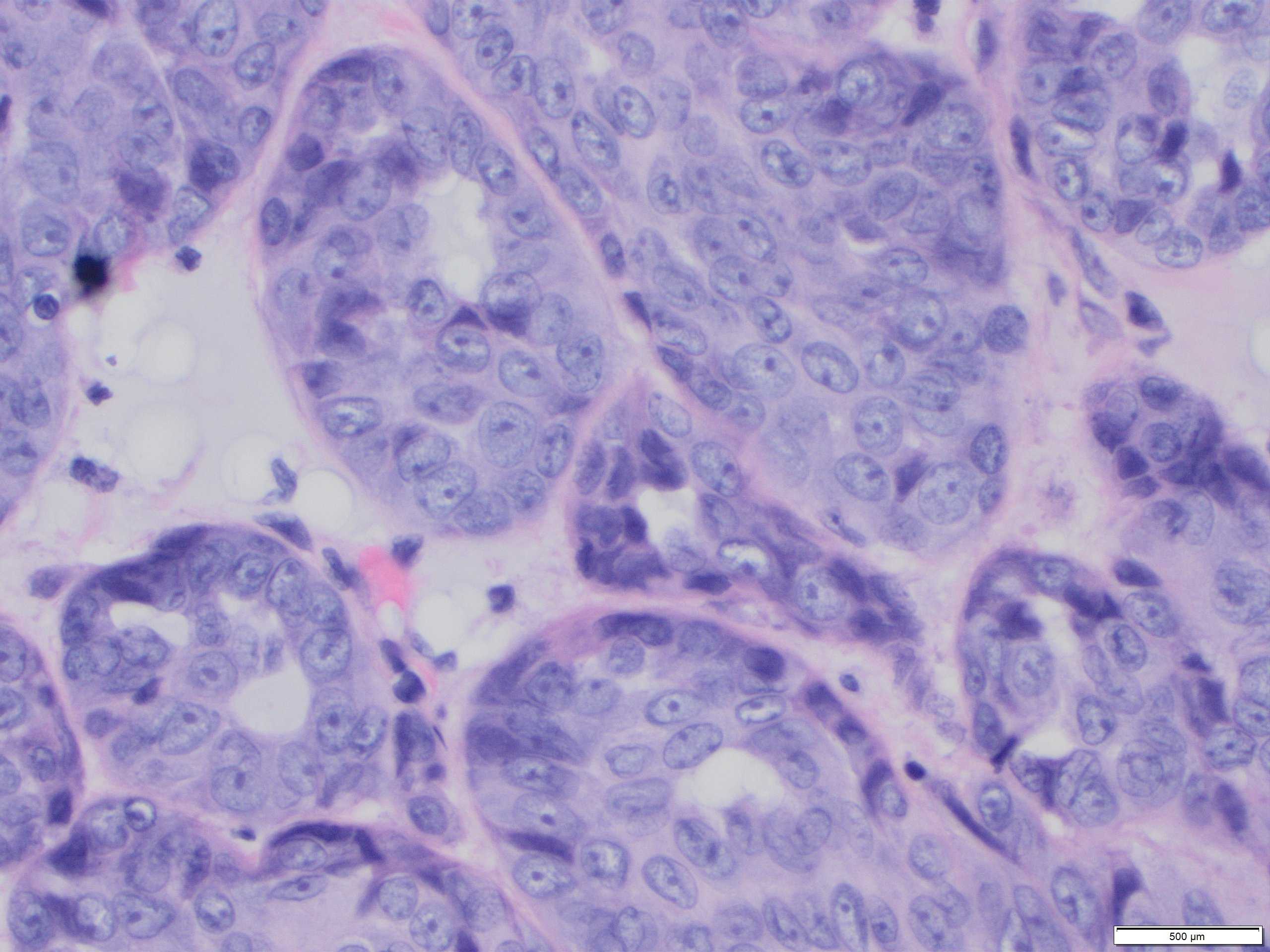
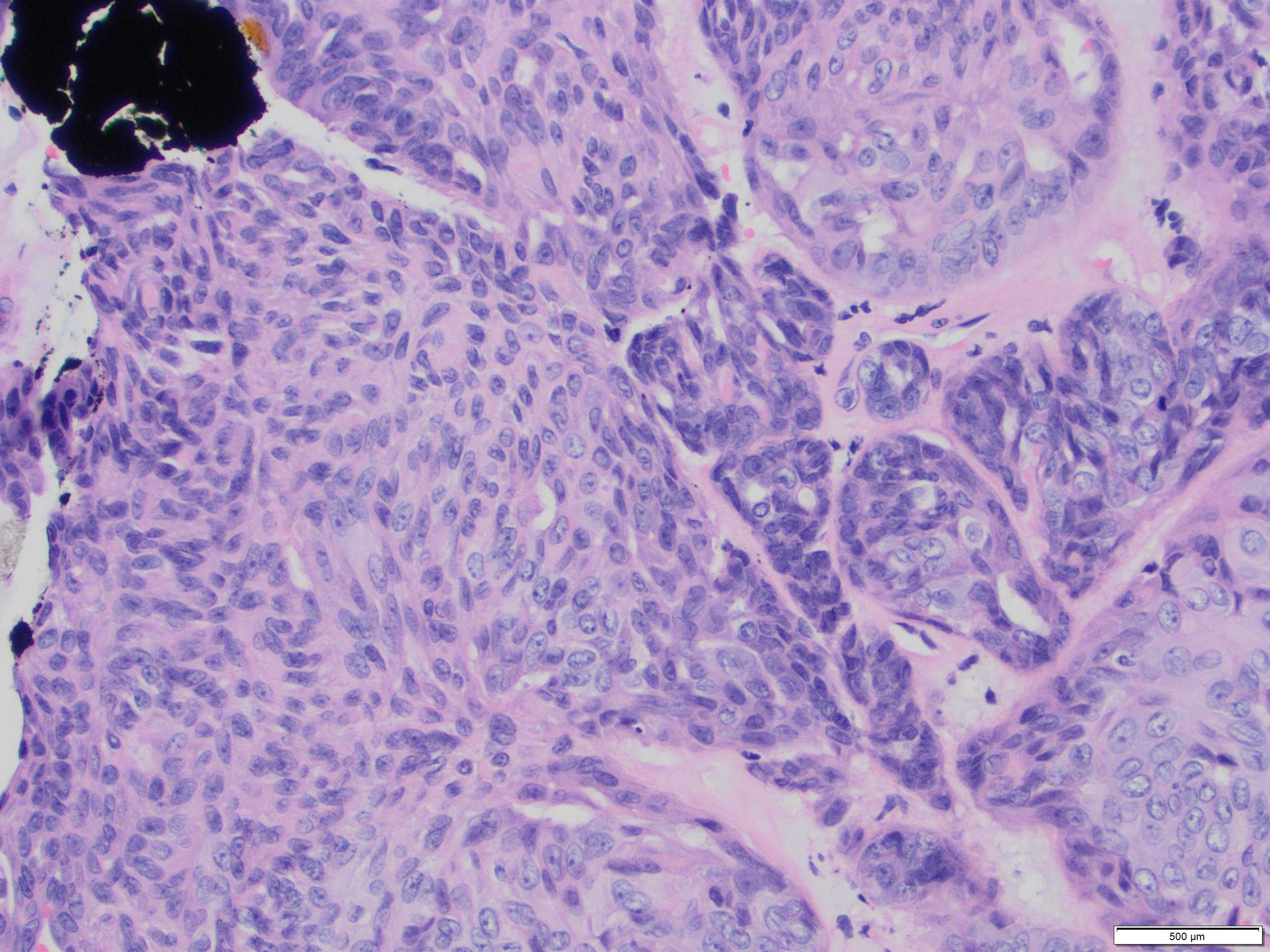
Classical benign AME comprises epithelial and myepithelial (MECs) with varying ratios within and between tumours. MECs usually dominate and are more numerous than the single basal layer component of the epithelial myoepithelial bilayer of normal breast lobules, adenosis nodules or simple papillomas. The cells are often small and uniform without cytological atypia or increased mitotic activity.
Malignant AME (M-AME) shows varied macroscopic appearances from a multilobulated, well-defined mass, similar to classic AME, to a poorly defined mass with infiltrative borders. Histological features of malignancy: overgrowth of the epithelial or myoepithelial component, mild to moderate cytological atypia, and increased mitotic activity with or without mildly infiltrative growth pattern, and/or focal necrosis.
M-AME may show an aberrant immunoprofile with loss of distinction of the dual cell population. The epithelial cell component may be positive for ER and EMA/MUC1 and show strong E-cadherin membrane expression. Complete absence of hormone receptor expression has been reported in 40% of AMEs, associated with nuclear atypia, necrosis and/or increased mitotic activity. HER2 is usually negative in these tumours.
Metastases have been reported in 16–32% of tumours classified as M-AME involving lung, brain, bone, thyroid, liver and axillary lymph nodes. The prognosis associated with M-AME with distant metastases is poor.
References:
1. Rakha E, Tan PH, Ellis I & Quinn C. Adenomyoepithelioma of the breast: a proposal forclassification. Histopathology2021,79,465–479.
2. Tan PH, Ellis IO. Epithelial myoepithelial tumours. In TheWHO Classification of Tumours Editorial Board ed.WHO classi-fication of tumours. 5th ed. Lyon: IARC Press, 2019; 39–48.
3. Geyer FC, Li A, Papanastasiou ADet al. Recurrent hotspotmutations in HRAS Q61 and PI3K-AKT pathway genes as dri-vers of breast adenomyoepitheliomas.Nat. Commun.