| 2003 Case #3 |  |
|
| The following patient was seen by Gorgas Course participants in the Outpatient Clinic of the Tropical Medicine Institute. |
 History: 42 yo male with 4 weeks of colicky epigastric pain worse after meals. No fever, icterus, diarrhea, or weight loss. No history of STDs, hepatitis, malaria. History: 42 yo male with 4 weeks of colicky epigastric pain worse after meals. No fever, icterus, diarrhea, or weight loss. No history of STDs, hepatitis, malaria.
Epidemiology: Policeman born in Cajamarca in the northern Andes of Perú before moving to Lima 20 years ago. Spent part of each year in his youth in a rural area with abundant contact with animals such as cows, pigs, dogs. Has traveled and worked in multiple coastal and jungle areas over the years. No ill contacts. No TB contact. No drugs, occasional alcohol, and no high-risk sexual activity. Physical Examination: Afebrile. Well-built, well nourished, appearing robust. No lymphadenopathy. Chest clear. An 8-10 cm protuberant abdominal mass was visible (indicated by the red arrow in the image) on inspection. The mass was non-tender, non-pulsatile, non-movable, well circumscribed on its anterior aspect and had a rubbery but not hard consistency. Normal rectal and genital exam. Laboratory Examination: Normal CXR. Hematocrit 42. WBC 8.9. 72 neutrophils, 1 band, 18 lymphs, 7 monocytes, 2 eosinophils. Liver function normal. HIV negative. Upper endoscopy - mild chronic gastritis. H. pylori positive.
|
| 2003 Case #3 Diagnosis& Discussion |
|
|
| (Links to Other 2003 Cases are at bottom of this page) | ||
| Diagnosis: Massive hydatid cyst due to Echinococcus granulosus. |
 Discussion: Based on the history and the physical examination, the differential diagnosis of a large cystic mass, apparently in the liver, is limited. Considerations would include neoplasms such as hepatocellular carcinoma, cystadenomas, or metastatic carcinoma. In general, these would present as stony hard and not rubbery masses. Of note though, is that Hepatitis B is hyperendemic in Amazonian regions of South America to the same extent as in many parts of Asia. Large hepatic cysts are often present in polycystic kidney disease but no other symptoms or signs were present in this case. Pyogenic or amebic liver abscesses would present with fever and a more aggressive course. Discussion: Based on the history and the physical examination, the differential diagnosis of a large cystic mass, apparently in the liver, is limited. Considerations would include neoplasms such as hepatocellular carcinoma, cystadenomas, or metastatic carcinoma. In general, these would present as stony hard and not rubbery masses. Of note though, is that Hepatitis B is hyperendemic in Amazonian regions of South America to the same extent as in many parts of Asia. Large hepatic cysts are often present in polycystic kidney disease but no other symptoms or signs were present in this case. Pyogenic or amebic liver abscesses would present with fever and a more aggressive course.
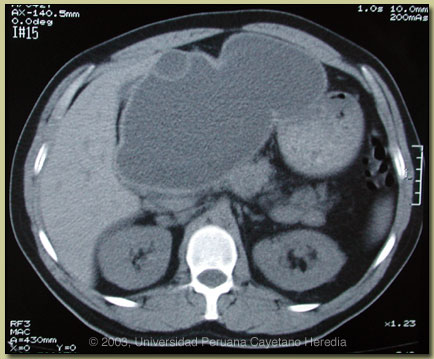
CT scan of the abdomen (see image at right) showed an uncomplicated 15 cm hepatic cyst with contents of liquid density replacing the left lobe of the liver. There is a small daughter cyst anteriorly. The endocyst and pericyst membranes are intact and without calcification. These CT findings indicate an active growing lesion with viable echinococcal scoleces in the contents. ELISA for E. granulosus was positive at 1.76 OD units (normal <0.5). Arc V immunodiffusion (higher specificity diagnostic test than ELISA) was also positive. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contamined by canine feces and become accidental intermediate hosts. Sheep are the normal intermediate hosts. Larval cysts expand slowly over years or decades becoming symptomatic as they impinge on other structures by virtue of their size. The cysts contain hundreds of viable scoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The germinal membrane lining the cyst produces new scoleces on an ongoing basis. Each scolex is capable of becoming a new daughter cyst either within the original cyst or elsewhere should the original cyst rupture or be ruptured. Hydatid disease is common in sheep-raising areas worldwide. Most primary infections involve a single cyst. 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 15% will also have a hepatic cyst. A primary hydatid cyst palpable on physical examination, such as is seen with our patient, is uncommon. Serology is usually positive with hepatic cysts but sensitivity drops below 50% with solitary pulmonary cysts even when the cyst is large. Possible treatment options in this case would include observation, medical therapy alone with albendazole, percutaneous drainage, or complete surgical resection. Observation of this superficial and very large cyst would carry the significant chance of a catastrophic rupture (with seeding of the peritoneum with viable scoleces) due to incidental blunt trauma. Medical therapy alone has had 30-70% success rates in various case series but success is most often with cysts less than 10 cm and many studies have excluded larger cysts such as this. Although there is little published data, it is the experience of many clinicians who have treated large numbers of patients that albendazole therapy of large tense cysts such as this significantly softens the capsule increasing the risk of spontaneous rupture or of slow leakage (can cause anaphylaxis). Percutaneous Aspiration Instillation (of a scolicidal solution) and Reaspiration (PAIR procedure) is increasingly used and recommended worldwide for uncomplicated cysts. This procedure is not currently available in Perú but would likely be the procedure of choice in an area where an experienced operator was available. Given the large size (>10 cm) of the cyst, we have recommended surgical resection which should be straightforward given the location of his cyst. Perioperative coverage with albendazole should be considered to cover the possibility of intraoperative spills. Nevertheless, some surgeons are reluctant to do this because of a feeling that albendazole softens the cyst wall and makes the surgery more difficult. Most surgeons inject hypertonic saline or other scolicidal agent (e.g., cetrimide) intraoperatively prior to cyst removal to kill viable scoleces. This should not be done in cases where there is any chance of the cyst having eroded into the biliary tree as the scolicidal agent will induce a sclerosing cholangitis.
|