| 2004 Case #6 |  |
|
| The following patient was seen on the 36-bed infectious/tropical disease unit of the Tropical Medicine Insitute in Lima. |
 History: 49 yo male with 3-month history of non-healing wound over the right retro-auricular area after an injury caused by an adobe brick. Slow progression of necrosis to the ear itself with liquid and purulent discharge from multiple sinus tracts. No fever, no headache, no neurological symptoms. Only local care received. History of periodic convulsions since age of 8 with no previous care or workup. Last seizure 2 days prior to admission. Patient is a heavy drinker. History: 49 yo male with 3-month history of non-healing wound over the right retro-auricular area after an injury caused by an adobe brick. Slow progression of necrosis to the ear itself with liquid and purulent discharge from multiple sinus tracts. No fever, no headache, no neurological symptoms. Only local care received. History of periodic convulsions since age of 8 with no previous care or workup. Last seizure 2 days prior to admission. Patient is a heavy drinker.
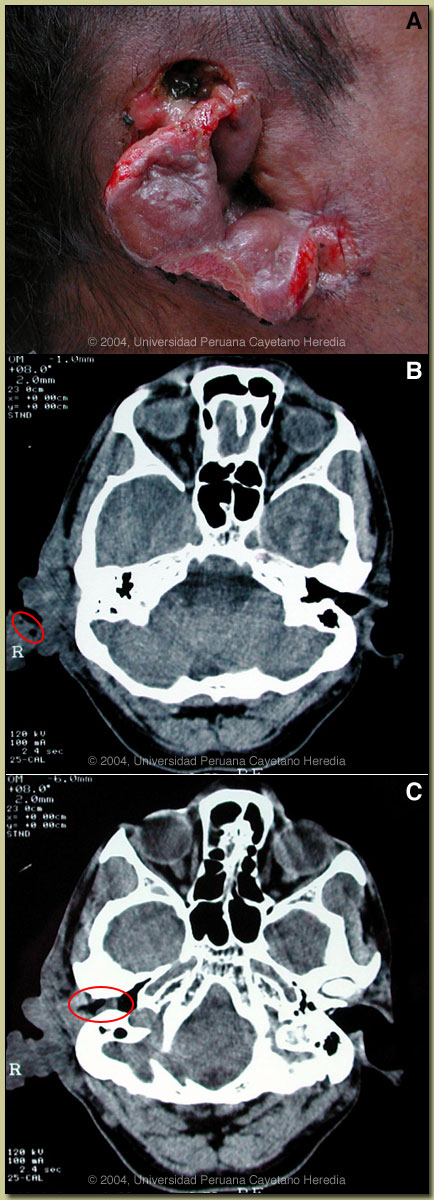
Epidemiology: Farmer; born and lives in the Cuzco area in the Andean highlands. No history of TB or HIV risk behavior. Physical Examination: Afebrile. Normal vital signs. Normal CNS examination. Wound is shown in image A. Laboratory Examination: Hematocrit 32%, WBC 8400, 68% polys, 8% eos; AST 32, ALT 31. Chest x-ray normal. CT scan of the head shows a soft-tissue mass of the skin and soft tissue in the right auricular area corresponding to the physical examination with several areas of subcutaneous emphysema [see image B]. There is a collection in the right external ear canal [see image C].
|
| Diagnosis: Infestation (myiasis) due to Cochliomyia hominivorax (the new world screwworm). |
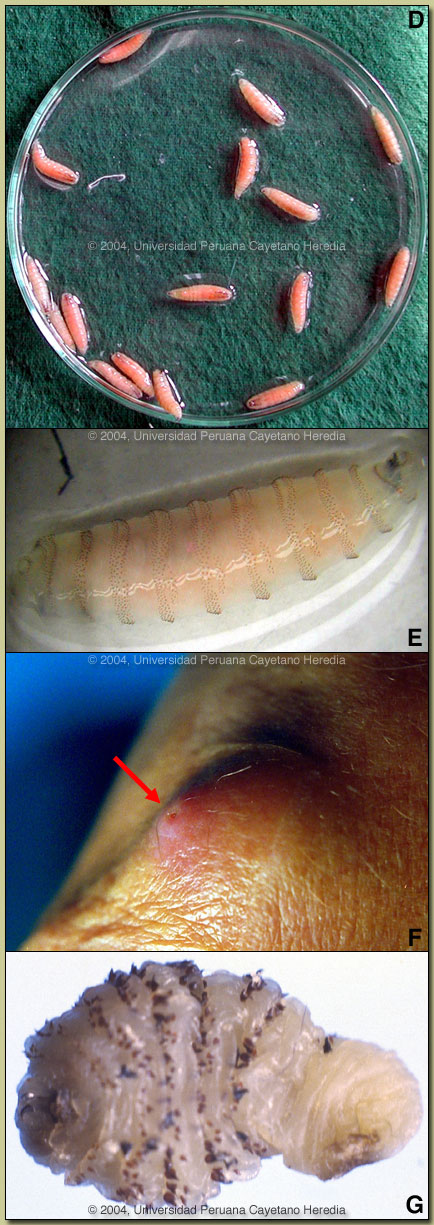 Discussion: After removing most of the necrotic tissue, approximately 20 live maggots were removed [see image D]. On further questioning the patient related that similar larvae had been discharged from the wound on several occasions beginning perhaps a month after the initial trauma. In reviewing the CT [see red circle, image B], the subcutaneous emphysema likely represents larval tracks in the tissue. The maggots are fourth stage Cochliomyia hominivorax [see image E]. The distinctive features of Cochliomyia are: smooth external aspect (opposite to hairy maggots), pigmented (other species are unpigmented) dorsal tracheal trunks, and two features difficult to observe in the present image; open peritreme (at the tail) and posterior spiracles not in cavity. Discussion: After removing most of the necrotic tissue, approximately 20 live maggots were removed [see image D]. On further questioning the patient related that similar larvae had been discharged from the wound on several occasions beginning perhaps a month after the initial trauma. In reviewing the CT [see red circle, image B], the subcutaneous emphysema likely represents larval tracks in the tissue. The maggots are fourth stage Cochliomyia hominivorax [see image E]. The distinctive features of Cochliomyia are: smooth external aspect (opposite to hairy maggots), pigmented (other species are unpigmented) dorsal tracheal trunks, and two features difficult to observe in the present image; open peritreme (at the tail) and posterior spiracles not in cavity.
Myiasis is defined as the infestation of humans or other vertebrates with larvae of Diptera (or true flies), with the larvae feeding on the host?s living or necrotic tissue. Cochliomyia hominivorax is an obligate parasite and an extremely destructive species whose larvae only feed on viable tissues in live hosts. The female fly lays a batch of 10-500 eggs at the edge of any type of skin wound, no matter how small the wound is. This includes tick bites and navals of newborn animals or humans. In addition eggs may be laid on mucous membranes including vagina, mouth or nose. The highly invasive larvae rapidly produce deep lesions that may be 5 cm or more deep. The spines may be used as anchors, making removal difficult. The odor of the lesion attracts other gravid females so that wounds may contain hundreds or thousands of larvae. When mature, the larvae fall from the host to pupate in the soil and develop into adult flies. The cycle takes about 3 weeks but may be several months in cooler climates such as in the Andes. The original description of human infestation with screwworm was in 1858 in prisoners on Devil?s Island in French Guiana. Coquerel described a fatal outcome in 3 of the 6 men (hominivorax means ?man-eater?) involved and screwworm was said to be responsible for hundreds of deaths over the years there. Cattle are the preferred host for larvae but all warm-blooded animals, including humans, seem at risk. Screwworm is a devastating agricultural disease and remains one of the major causes of morbidity and mortality amongst livestock in tropical and sub-tropical regions. Once an animal becomes infested with screwworm, death is generally inevitable unless the wound is cured. Large programs in the 1970s and 1980s using sterile male flies have eradicated new world screwworm from the United States. Similar programs are ongoing in Mexico and Central America. The current southern range extends to Uruguay and northern Chile. Any case of human Cochliomyia hominivorax myiasis imported into the USA is regarded as a public health emergency by the US Department of Agriculture. A case several years ago in Alabama resulted in a large-scale quarantine of an entire neighborhood until application of appropriate pesticide could be effected. A bioterrorism potential is apparent. Chrysomya bezziana, the old world screwworm is widely distributed outside the Americas. In travelers, furuncular myiasis due to Dermatobia hominis, the human botfly, is a much more common form of myiasis. A larva penetrates intact skin. The larva lives only in the subdermis, is most often single, and appears as a furuncle or boil characterized by a small punctum through which the larva obtains oxygen [see arrow, image F; from Gorgas Teaching Files]. Occlusion of the respiratory punctum such as with paraffin or petroleum jelly often causes the pear-shaped larva [see image G] to come out and is curative. Professor Hugo Lumbreras, the founder of our Tropical Medicine Institute, used to teach of the traditional approach to myiasis in Perú, which involved the occlusion of the entrance of the wound by a solution made from basil leaves, the odor of which forced the larvae out of the wound. Because of the highly invasive nature of Cochliomyia hominivorax, a more extensive debridement under anesthesia is planned for our patient. Due to the suppurative superinfection, the patient is receiving IV clindamycin. At our institute we see about 10 outpatients per year with screwworm infestation and over the last 10 years 7 have required hospitalization. Dermatobia hominis occurs in Perú but is generally not serious enough to warrant referral to an institution such as ours.
|
| The following patient was seen on the 36-bed infectious/tropical disease unit of the Tropical Medicine Insitute in Lima. |
| History: 49 yo male with 3-month history of non-healing wound over the right retro-auricular area after an injury caused by an adobe brick. Slow progression of necrosis to the ear itself with liquid and purulent discharge from multiple sinus tracts. No fever, no headache, no neurological symptoms. Only local care received. History of periodic convulsions since age of 8 with no previous care or workup. Last seizure 2 days prior to admission. Patient is a heavy drinker.
Epidemiology: Farmer; born and lives in the Cuzco area in the Andean highlands. No history of TB or HIV risk behavior. Physical Examination: Afebrile. Normal vital signs. Normal CNS examination. Wound is shown in image A. Laboratory Examination: Hematocrit 32%, WBC 8400, 68% polys, 8% eos; AST 32, ALT 31. Chest x-ray normal. CT scan of the head shows a soft-tissue mass of the skin and soft tissue in the right auricular area corresponding to the physical examination with several areas of subcutaneous emphysema [see image B]. There is a collection in the right external ear canal [see image C].
|