| 2005 Case #8 |  |
|
| The following patient was seen by course participants in the Outpatient Clinic of the Tropical Medicine Institute. |
 History: 16-month old child with onset of a single non-tender but pruritic lesion on the ear lobe 2 months earlier. Over the next weeks similar lesions developed on the face and limbs. No fever, otherwise thriving and developing normally. History: 16-month old child with onset of a single non-tender but pruritic lesion on the ear lobe 2 months earlier. Over the next weeks similar lesions developed on the face and limbs. No fever, otherwise thriving and developing normally.
Epidemiology: Born and living in Lima but traveled 5 months earlier to Apurimac, a town in an Andean valley in south central Peru. A short febrile illness during that trip was treated with an unknown antibiotic. Normal vaginal delivery, all maternal prenatal screening bloodwork normal. All childhood immunizations are up to date. Physical Examination: Afebrile. Red papules [Image A] on both ear lobes, right lower eyelid, forehead, and upper and lower lips. Bilateral cervical adenopathy. Laboratory Examination: No bloodwork performed. Biopsy sent. |
| Diagnosis: Verruga Peruana - the chronic form of bartonellosis due to Bartonella bacilliformis. [see also Gorgas Case 2005-01, Acute Bartonellosis]. |
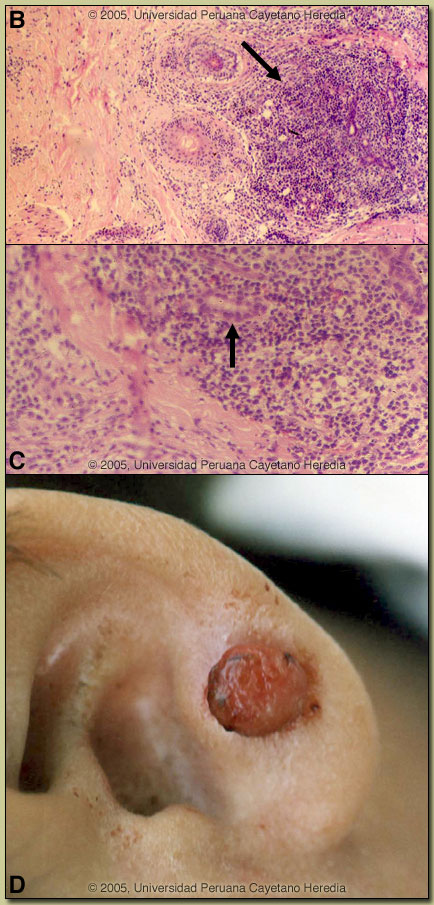 Discussion: In addition, to the classical clinical lesions, the biopsy of the earlobe lesion showed the characteristic proliferation of capillaries [Image B] with thickened endothelial cells [Image C, arrow] with an interspersed inflammatory infiltrate of lymphocytes and macrophages. Discussion: In addition, to the classical clinical lesions, the biopsy of the earlobe lesion showed the characteristic proliferation of capillaries [Image B] with thickened endothelial cells [Image C, arrow] with an interspersed inflammatory infiltrate of lymphocytes and macrophages.
Acute bartonellosis (Oroya fever) has been discussed [Gorgas Case 2005-01]. In those untreated patients that have inapparent acute bacteremic phases or survive the primary infection, a chronic eruptive phase occurs several months later. Skin lesions, called Verruga Peruana, are most commonly miliary in nature with multiple 1-4 mm papular, erythematous round lesions that are often pruritic. These are loaded with bacteria. The differential diagnosis of the clinical lesions include pyogenic granuloma, hemangioma (would have few lesions), Kaposi?s sarcoma, and a variety of other subcutaneous tumors. The lesions are clinically and histologically very similar to those that occur with Bacillary Angiomatosis which is caused by infection with Bartonella henselae (the agent of cat-scratch disease) or Bartonella quintana in HIV or other severely compromised patients. Our patient had no history of cat contact. The distribution of Bartonella bacilliformis, which is transmitted by the bite of the Lutzomyia verrucarum sandfly is restricted to the inter-Andean valleys of Peru and Ecuador where this child had traveled several months earlier. In endemic communities in these valleys, the highest rates of infection are in children <5 years old, and there is a linear decrease in incidence with increasing age. Household clustering clearly occurs. Besides for the presentations shown here and in Gorgas Case 2005-01 multiple other clinical presentations may occur. Recent data suggest that significant subclinical infection may be occurring in endemic areas. Though blood cultures were negative in the current case, B. bacilliformis can be isolated in blood cultures (special conditions required) from about 10% of those with chronic disease (verrugas) indicating that a minority of patients may be acting as an ongoing reservoir of infection. Recent in vitro data confirm that B. bacilliformis is sensitive to most antibiotics including penicillins (including Penicillin G and ampicillin), cephalosporins, aminoglycosides, chloramphenicol, macrolides, tetracyclines, and quinolones [Antimicrob Agents Chemother. 2004 Jun;48(6):1921-33]. Ceftriaxone has the best MIC values of all antibiotics tested. In the past chloramphenicol has been used extensively in Peru for acute disease but a proportion of those treated may still go on to develop verrugas and chronic disease. Recently, ciprofloxacin is more frequently used for acute disease. For Verruga Peruana, the most published experience has been with rifampin which has been used for over 30 years in Peru. More recently both ciprofloxacin and azithromycin have been utilized for the chronic lesions although published comparative studies have yet to be published. Our patient was treated with 10 days of rifampin with good resolution of lesions. The resolving earlobe lesion is shown in Image D. Reference: Maguina C., et al. Bartonellosis (Carrion's Disease) in the Modern Era. Clin Infect Dis. 2001 Sep 15;33(6):772-9. |