| 2006 Case #1 |  |
|
| The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Peru. For the sixth consecutive year, we are pleased to share interesting cases seen by the participants each week during the February/March course offerings. Presently the 9-week Gorgas Course in Clinical Tropical Medicine is in session. New cases will be posted every Monday for the next nine weeks. Each case includes a brief history and digital images pertinent to the case, followed by a second page with the diagnosis and brief discussion. |
| The following patient was seen in the Medicine Service at the 450-bed Cayetano Heredia National Hospital. |
 History: 20 yo male with a 3-week history of high fever, headache, insomnia, epistaxis, diffuse abdominal pain and 3-6 dark black loose stools per day. One week after the onset of illness, the patient was seen in a local hospital where oral chloramphenicol was prescribed but was stopped after 3 days when no improvement resulted. History: 20 yo male with a 3-week history of high fever, headache, insomnia, epistaxis, diffuse abdominal pain and 3-6 dark black loose stools per day. One week after the onset of illness, the patient was seen in a local hospital where oral chloramphenicol was prescribed but was stopped after 3 days when no improvement resulted.
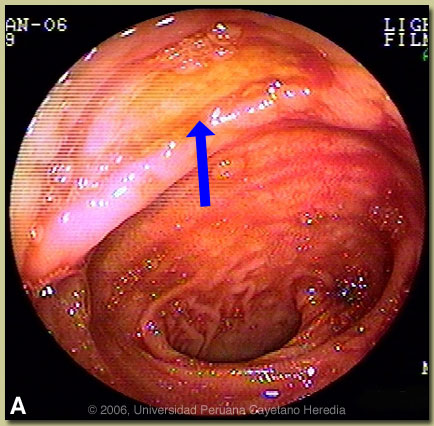
Epidemiology: Single, bisexual, born and lives in Lima where he works as a laborer. No recent travel. Father with TB 10 years ago, no history of receiving prophlaxis. Physical Examination: T 38.5°C, pulse 100, respirations 22, BP 110/75. Uncomfortable looking with no icterus, no rash. Small non-tender cervical, axillary, and inguinal lymph node enlargement. Chest clear, cardiovascular normal. Mild diffuse abdominal tenderness, no peritoneal signs, no hepatosplenomegaly. Laboratory Examination: Hct. 34% on admission, to 28% the next day. WBC 5300, 0% bands, 59% neutrophils, 1% eos, 4% monos, 36% lymphs, platelets 246K. INR 1.25. Total bili 0.5 mg/dl, alk phosp 92, ALT 129, AST 344, LDH 1012. Normal glucose and electrolytes. HIV negative. Chest X-ray normal. Abdominal ultrasound disclosed mild splenomegaly, otherwise normal. Blood cultures with no growth at 2 weeks. Widal test; O antigen negative (zero), H 1/80. Brucella agglutinins negative. Colonoscopy was performed 3 days after admission, showing 2 lesions in the ileum. The lesion in Image A is located 10 cm from the ileo-cecal valve. A biopsy was taken.
|
| Diagnosis: Typhoid fever complicated by gastrointestinal bleeding and intestinal ulceration. |
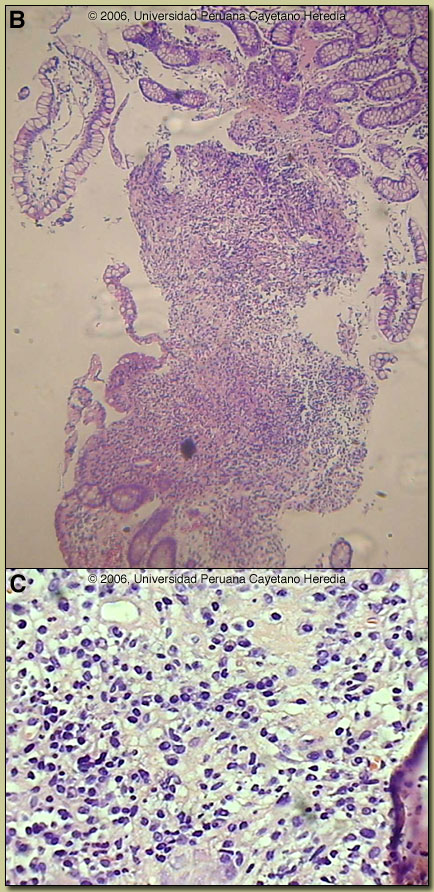 Discussion: A bone marrow aspirate taken on admission grew Salmonella enterica var typhi susceptible to ampicillin, chloramphenicol, quinolones, and third generation cephalosporins except for ceftazidime. Stool cultures were negative. Biopsy of the 1 cm long ileal ulcer with raised borders and yellow material at the base showed ulcerated ileal mucosa [Image B] with a dense inflammatory infiltrate in the lamina propria. The predominant infiltrate consists of aggregates of histiocytic cells, and is accompanied by some lymphocytes and plasma cells [Image C]. The typical histopathological finding of so-called ?typhoid cells?, tissue infiltration by aggregates of histiocytes containing bacteria and degenerating lymphocytes, was not seen in this case. Discussion: A bone marrow aspirate taken on admission grew Salmonella enterica var typhi susceptible to ampicillin, chloramphenicol, quinolones, and third generation cephalosporins except for ceftazidime. Stool cultures were negative. Biopsy of the 1 cm long ileal ulcer with raised borders and yellow material at the base showed ulcerated ileal mucosa [Image B] with a dense inflammatory infiltrate in the lamina propria. The predominant infiltrate consists of aggregates of histiocytic cells, and is accompanied by some lymphocytes and plasma cells [Image C]. The typical histopathological finding of so-called ?typhoid cells?, tissue infiltration by aggregates of histiocytes containing bacteria and degenerating lymphocytes, was not seen in this case.
Typhoid fever is a systemic febrile illness caused by Salmonella enterica sub-species enterica serotype Typhi. Prolonged fever, sustained bacteremia, and intracellular multiplication of the bacteria within mononuclear phagocytic cells of the liver spleen, lymph nodes, and Peyer?s patches are hallmarks of the infection. Paratyphoid fever is a pathologically similar but milder disease caused by a number of other serotypes of Salmonella. Transmission is usually via contaminated food and water. S. typhi can survive for weeks in water, ice, sewage and on inanimate objects. Stool from chronic carriers can contain from 106 to 109 organisms. Ingested bacteria invade small intestinal epithelial cell and are initially internalized in intestinal lymphoid cells and draining mesenteric lymph nodes. At the end of an incubation period, which is generally 7-14 days but can vary from 3-60 days, clinical disease heralds the onset of the bacteremic phase of the infection. Bacteria may invade any organ but most commonly invade mononuclear cells within liver, spleen, bone marrow, gallbladder and Peyer?s patches. Involved Peyer?s patches are generally in the terminal ileum within 60 cm of the ileo-cecal junction and in the cecum itself. Without treatment, after about 7-10 days of illness, necrosis and sloughing of the overlying mucosa may result with ulcer formation and more rarely intestinal perforation. Ulcers are usually 1 cm or less in size and most often solitary. Most patients are children and young adults under 25. Clinical manifestations are protean and non-specific but almost always include fever and headache. The headache often results in insomnia. Fever is initially low-grade but by the second week is high (39 to 40°C) and sustained. There may be intermittent confusion and many patients have an apathetic affect. Complications occur in 10-15% and are more frequent in patients who have been ill for 2 weeks or more. While a large number of complications have been described, clinically obvious gastrointestinal bleeding (10% of all patients), intestinal perforation (1-3% of hospitalized patients), and encephalopathy are the most common. GI bleeding is serious in 2% of all cases. Based on the colonoscopic findings other, but less likely, diagnoses in this case would be intestinal tuberculosis or yersinia infection. Entameba histolytica and Balantidium coli infection cause ulcers and perforation but would only be found in the colon. Peripheral blood cultures are positive in 40-80% of patients only reaching higher yields if 15 ml of blood are cultured because of the low numbers of organisms in peripheral blood with 80% of those being intracellular. As demonstrated in this case, culture of bone marrow increases the yield to >95% and may remain positive even in the face of several days of antibiotic therapy. Blood cultures yield decreases after the first week of illness. Stool cultures are positive in 30% of cases of acute typhoid fever. The Widal test remains controversial because of highly variable sensitivity, specificity and predictive values in different settings. The negative Widal test in this patient with 3 weeks of illness reinforces this point. Drug resistance in Latin America has not occurred to the same extent as in Asia and other areas of the world. Most of the typhoid in Peru remains sensitive to ampicillin, chloramphenicol, and trimethoprim/sulfa. Nevertheless, oral quinolones remain the treatment of choice for uncomplicated typhoid due to insignificant rates of relapse and chronic carriage as well as faster times to fever resolution of quinolones compared to the older drugs. Quinolone resistant S. typhi, which has become highly prevalent in Asia, has not emerged in Latin America, so that empiric quinolone therapy can be initiated without reservation in those who acquire infection in Latin America. In febrile patients, clinicians often characterize a non-response of fever after 48 hours as an antibiotic failure and switch drugs. In typhoid fever, response to quinolones most often does not occur until Day 4 or 5 and with chloramphenicol it is usually longer. This patient?s non-response to chloramphenicol after 3 days was mis-interpreted as a failure and he likely would have had an early cure had he completed his prescribed course. Many sources continue to list Peru as a highly endemic country for typhoid fever based on data and experience from the 1980s. The cholera epidemic that began in 1991 in Peru and other Latin American countries resulted in the implementation in Peru of many public health and infrastructure changes that had a dramatic bystander effect on typhoid fever incidence rates [Infect Dis Clin North A
|