| 2011 Case #1 |  |
|
|
The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Perú. For the eleventh consecutive year, we are pleased to share interesting cases seen by the participants that week during the February/March course offerings. Presently the 9-week Gorgas Course in Clinical Tropical Medicine is in session. New cases will be posted every Monday/Tuesday for the next nine weeks. Each case includes a brief history and digital images pertinent to the case. A link to the actual diagnosis and a brief discussion follow. David O. Freedman & Eduardo Gotuzzo |
| The following patient was seen in the inpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital. |
|
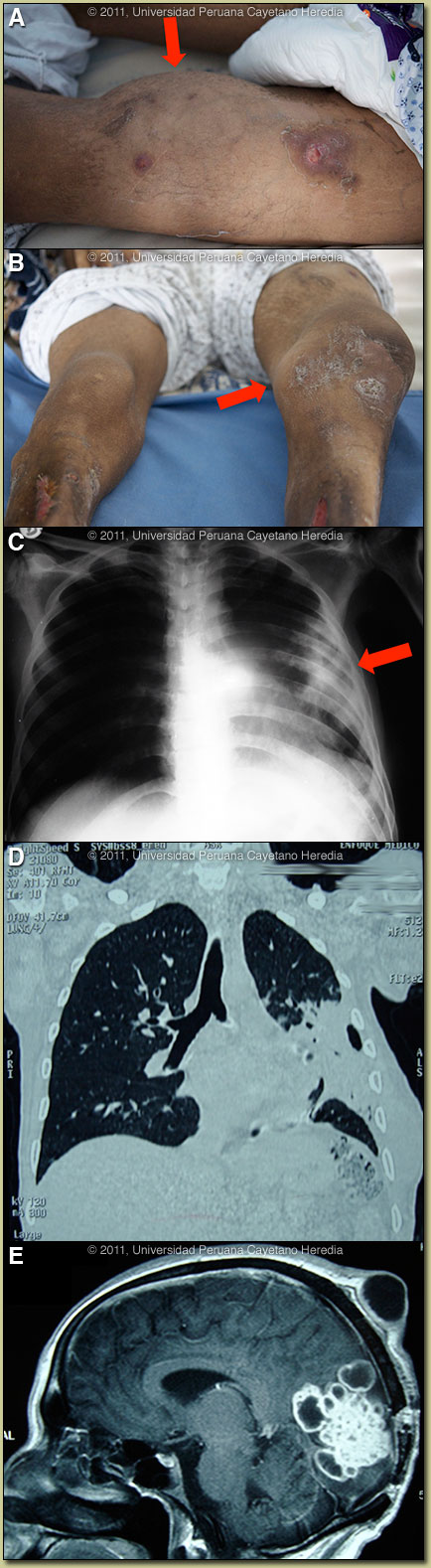
Epidemiology: Born and lives now in Lima. 1983-2003 lived in the jungle as a suspected narcotics trafficker. Incarcerated for 3 years in the jungle and the past 1 year in Lima. Known TB contacts. Alcohol abuser. Physical Examination: T 37°C, RR 16, HR 90, BP 110/60. Alert x 3, Glasgow score: 15. Extensive nodular subcutaneous lesions and subcutaneous masses on the scalp, thorax and on the limbs [Image A]. Left knee arthritis with extensive effusion [Image B]. Remote memory loss, blurred vision, no meningeal signs. Normal fundi. Laboratory: (on admission to our hospital) Hematocrit 21. WBC 13,5 (92 PMN, 0 Eos, 3 M, 15L). Plt. 527,000, Bili normal, Alk P 220, GGT 66. VDRL, HIV, HbSAg negative. Current CXR, Chest CT, and brain MRI are shown [Images C, D, E]. Brain biopsy 3 months earlier at another hospital had shown acid fast organisms with negative culture for MTB or bacteria.
|
| Diagnosis: Disseminated nocardiosis. |
 Discussion: An aspirate of a right forearm abscess grew a weakly acid-fast organism compatible with Nocardia species when cultured aerobically [Images F, G]. Further workup is in progress. In addition, as aspirate of the knee joint grew Nocardia. The culture was negative for mycobacteria and did not grow anaerobically. Review of the images indicated that both the scalp and chest-wall lesions were contiguous with internal foci of infection. The brain MRI is highly diagnostic of nocardiosis. Discussion: An aspirate of a right forearm abscess grew a weakly acid-fast organism compatible with Nocardia species when cultured aerobically [Images F, G]. Further workup is in progress. In addition, as aspirate of the knee joint grew Nocardia. The culture was negative for mycobacteria and did not grow anaerobically. Review of the images indicated that both the scalp and chest-wall lesions were contiguous with internal foci of infection. The brain MRI is highly diagnostic of nocardiosis.
Although literature is limited, nocardiosis appears to present in the tropics in a similar way to non-tropical areas, though this is the first case we have seen in over 20 years in our tertiary care facility in Lima. Although M. tuberculosis infection would be at the top of the differential diagnosis list in the tropics at initial pulmonary presentation in this case, the spread to skin, joint and CNS would be unusual. Actinomycosis rarely presents in the CNS and actinomycotic skin lesions arise entirely by contiguous spread usually from a respiratory focus and that would not explain the hematogenous spread to the knee joint here. Endemic fungi (sporotrichosis, paracoccidioidomycosis) can present with skin nodules but these quickly ulcerate and would not remain nodular over a period of years. Some uncommon disseminated forms of L. brasiliensis exist but would not have pulmonary or CNS manifestations. Nocardia are aerobic, partially acid-fast, branching, filamentous, slow growing Gram-positive bacilli. Infection is acquired by direct inoculation or inhalation and spreads hematogenously from the lungs. Six basic forms of disease reported: pulmonary, systemic, central nervous system (rare), extrapulmonary, cutaneous, and actinomycetoma (often presenting as ‘madura foot’ in the tropics). Nocardiosis is mostly seen in severely immunosuppressed patients such as with HIV, organ transplantation, corticosteroid therapy, autoimmune conditions, COPD, and malignancy. TMP/SXT prophylaxis as used with many of these patients for a number of other infections does not seem highly protective against nocardiosis. The great majority of patients have a risk factor; our patient had a long history of alcoholism and incarceration. There are no therapeutic recommendations based on clinical trials. Usually, TMP/SMX is the primary choice for brain abscesses. For the disseminated form, as here, intravenous therapy should be for at least 2 months with at least 2 drugs, and with 3 drugs if there is CNS involvement. Our patient is now improving on TMP/SMX plus a third generation cephalosporin plus Amikacin. The plan is to complete oral therapy for at least 1 year.
|