 |
Gorgas Case 2024-8 |
|
The 2024 Gorgas Course participants saw the following patient in the pediatrics inpatient ward of Cayetano Heredia Hospital in Lima.
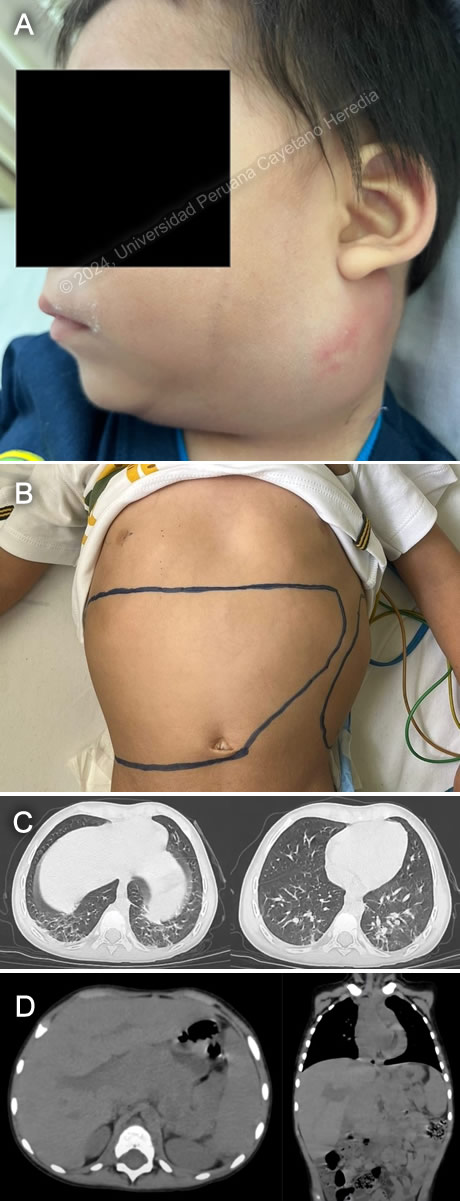 History: A 3-year-old male patient with no significant past medical history was transferred from the National Cancer Institute to Cayetano Heredia Hospital with seven weeks of fever, lymphadenopathies, and malaise. Seven weeks before admission, based on the information provided by the patient's mother, the patient had been feeling unwell with a fever of 38.5º C. Although the fever subsided partially with symptomatics, no other systemic symptoms were reported. Four weeks before admission, the fever persisted, and the mother noticed progressive swelling in the left cervical region that was painful to the touch. Three weeks before admission, the mother detected multiple mobile nodes in the neck and groin areas and progressive abdominal distension. On the day of admission, the patient was taken to the local hospital and then transferred to our National Cancer Institute for further evaluation of a presumptive lymphoproliferative disorder. Epidemiology: The patient was born in Villa Rica, a town in Pasco, in the high jungle of Peru. He has resided in that town for his entire life. His family is involved in coffee harvesting. His mother says he usually accompanies her in her activities, but most of the time, he stays at their humble home, which has basic amenities and a dirt floor. The child mostly eats soups and bananas. He has never traveled outside of his community before. Physical Examination on admission: HR: 138 bpm, RR: 35 bpm, T: 38.2°C, BP: 90/60, SatO2: 97% (breathing room air). The child appeared to be chronically malnourished and in good hygienic condition. The skin seemed pale and without swelling. A palpable lymph node on the left side of the neck, measuring 8 x 8 cm, was painful to the touch (Image A). Multiple lymph nodes were found in the retroauricular, submandibular, axillary, and inguinal regions, which were mobile and painless. There was mild swelling in the left periorbital region, and no injuries were found in the mouth. The abdomen appeared distended but non-tender. The liver was palpable 5 cm below the costal margin, indicating hepatomegaly. There was also splenomegaly (Image B). Overall, the rest of the examination was unremarkable. Laboratory: Hemoglobin was 9 mg/dL, and hematocrit was 28 %. WBC was 25100/uL with 0 bands, 17670 neutrophils, 2360 eosinophils, 180 basophils, 1280 monocytes, and 3640 lymphocytes. Platelets were 1 138 000/uL. Glucose 77 mg/dL, Creatinine 0.25 mg/dL. LDH was 326 UI/L. AST was 20 U/L. Sodium was 139 mEq/L, potassium was 4.87 mEq/L, chloride was 100 mEq/L, and ionic calcium was 1.2 mmol/L. HIV was negative. AFB from a gastric aspirate was negative three times. A CT scan from the chest (Image C) showed ground-glass opacities at both bases and reticulo-nodular opacities. Additionally, a CT scan from the abdomen (Image D) confirmed the presence of hepatosplenomegaly. Height-for-age: moderate chronic malnourishment (-3 S.D < Z < -2 S.D). Weight-for-age: moderate acute malnourishment (-3 S.D < Z < -2 S.D) UPCH Case Editors: Carlos Seas, Course Director / Jorge Nakazaki, Associate Coordinator |
|
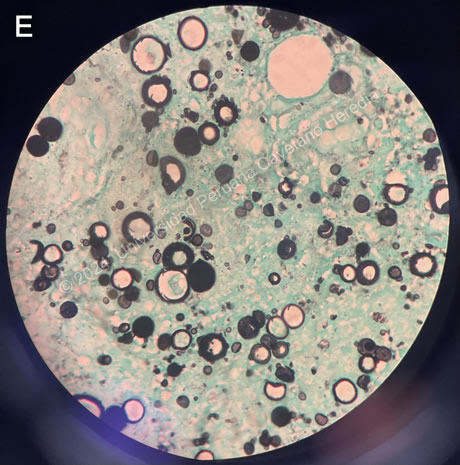
 Discussion: Based on the evaluation of clinical symptoms, epidemiological factors, medical images, and laboratory results, an aspirate biopsy of the neck tumor was decided upon. The results of the aspirate biopsy showed the presence of multiple fungal structures in the shape of a ship's wheel and "Mickey Mouse" with the Gomori-Grocott staining. These findings confirmed the diagnosis of paracoccidioidomycosis (Image E). Additionally, another slide showed chronic necrotizing granulomatous lymphadenitis. Paracoccidioidomycosis (PCM) is one of Latin America's most common systemic mycoses. It is mainly caused by the fungus Paracoccidioides brasiliensis. This fungal disease predominantly affects individuals in jungle rural areas of Central and South America. The disease is contracted through the inhalation of conidia in the air and is commonly found in male rural workers (1). It is most commonly contracted during the first two decades of life, with the highest incidence occurring between 10 and 20 years of age. PCM can be present in different forms, such as the juvenile form in our case. The acute/subacute form of the disease, known as the juvenile type, affects both boys and girls equally and has a prevalence of 5% to 25% of cases. It can also affect young adults and those between 30 and 40 (2,3). The disease takes around four to twelve weeks to evolve and usually affects the lungs, although it can also spread to other parts of the body, such as the skin, mucous membranes, lymph nodes, and internal organs (3). According to several studies, the most commonly reported symptoms are generalized or localized lymphadenopathy, fever, weight loss, hepatosplenomegaly, lytic lesions in bones, jaundice, and cutaneous mucosal involvement. Pulmonary involvement is less common in comparison to the adult chronic form of the disease (4). In laboratory tests, the most frequently found conditions are anemia, leukocytosis with left shift added, and significant eosinophilia in 30% to 50% of cases (5). Paracoccidioidomycosis is typically diagnosed through clinical evaluation, imaging studies (such as chest X-ray or CT scan), and laboratory tests. The laboratory tests aim to detect the presence of the fungus or its components in specimens such as sputum or tissue samples. These tests are based on identifying the yeasts of Paracoccidioides brasiliensis, which are multi-sized yeasts with multiple budding, in fresh samples, such as sputum, scrapings of skin lesions, or lymph node aspirate. Additionally, observing these yeasts in a biopsy of skin, mucosa, or lymph nodes can also be helpful for diagnosis. For a biopsy, Gomori-Grocott or PAS staining is used. Tests based on identifying antibodies and antigens are also beneficial for diagnosing and monitoring the response to therapy (6). The usual treatment for fungal infections involves using antifungal medications such as itraconazole or sulfonamides for an extended period. In severe cases, amphotericin B may be used. For mild to moderate forms, itraconazole is the first line of treatment administered for 9 to 18 months, with an average of one year. For severe and disseminated forms, amphotericin B is used for 2 to 4 weeks, followed by an azole for a prolonged period. Trimethoprim/sulfamethoxazole is an option for pediatric patients due to its good bioavailability and syrup formulation (5,6,7). References |