 |
Gorgas Case 2024-9 |
|
This is our last Case of the Week for the Gorgas Diploma Course of 2024. Publishing these case reports would not be possible without the assistance of an extremely dedicated group of people. We would like to thank in particular: Dr. Carlos Seas, Co-Director and Clinical Rounds Coordinator for the Gorgas Courses, Dr. German Henostroza, Co-Director and Dr. Jorge Nakazaki for case selection and coordination of case summaries and images.
We hope you have enjoyed the 2024 series of live cases each week from Perú. The following patient was seen on clinical rounds in the Social Security Hospital of Cuzco, Peru, during the Gorgas Course in 2024. 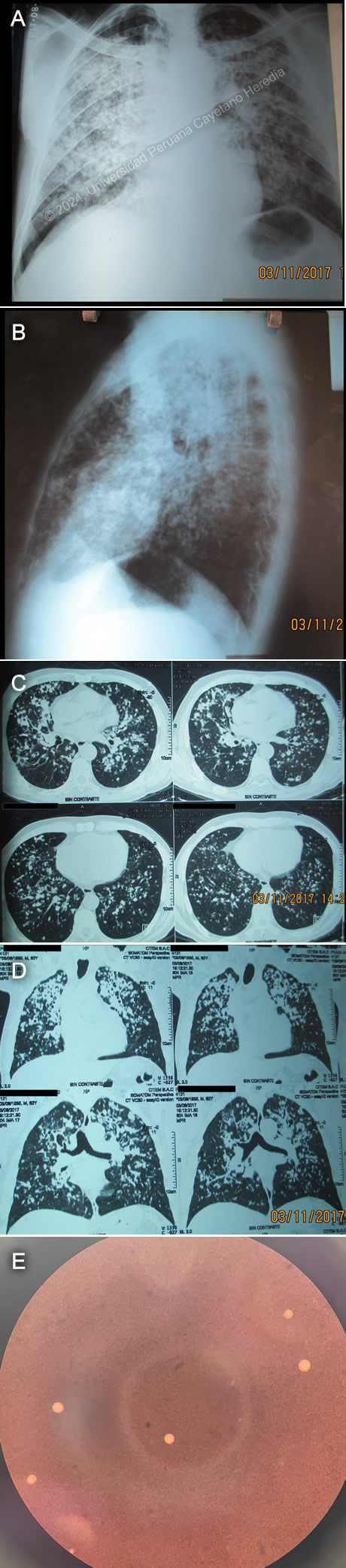 History: A 62-year-old male patient presented with a 3-month history of productive cough with yellowish sputum and multiple oral lesions. Three months before admission, the patient presented a productive cough with yellowish sputum without hemoptysis or other upper respiratory symptoms. This was associated with the appearance of multiple well-defined painful oral ulcers. Subjective fevers were added one month before admission, predominantly at night. This was associated with a 10kg weight loss. Epidemiology: The patient was born in a rural town in the highlands of Cusco, Peru. He grew up and lives in the city of Tambopata in the rainforest of Madre de Dios, where he works as a farmer. Twenty years before admission, he was diagnosed with cutaneous leishmaniasis and received incomplete treatment with pentavalent antimonials. Ten years before admission, his wife passed away from complications of pulmonary tuberculosis. Physical Examination on admission: BP: 85/60, HR: 98x’, RR: 37x’, T°:36°C. The patient looked cachectic with marked skin pallor. He had well-defined ulcers in the hard palate, but no skin lesions were noted. On auscultation, he had diffuse rhonchi and fine crackles in both lung fields. An umbilical hernia was found with no signs of incarceration. The rest of the exam was within normal limits. Laboratory: Hemoglobin was 14.8 mg/dL, leucocytes 6180 cells/mL with 4040 neutrophils, 120 eosinophils, no basophils, no monocytes, and 1380 lymphocytes. Platelets were 397 000/mm3. Urea was 36 with a Creatinine of 0.8 mg/dL. AST and ALT were 27 and 37 U/L, respectively. Sodium was 139 mEq/L, potassium 3.6 mEq/L, chloride 109 mEq/L. An ABG revealed a pH of 7.46, pC02 24 mmHg, bicarbonate 17 mmol/L, pO2 55 mmHg, and SpO2 82%. A lumbar puncture revealed an opening pressure of 16 cmH20, 1 lymphocyte, no RBCs, and glucose of 44 with serum glucose of 90. CSF in VDRL, India ink, and Cryptococcal latex agglutination assay were negative. Blood cultures for aerobic and anaerobic bacteria were negative. Acid-fast bacilli (AFB) stains and mycobacterial cultures on sputum, stools, and urine were negative. A peripheral blood smear did not reveal intraerythrocytic organisms. Serologies for HIV, hepatitis B, hepatitis C, and syphilis were negative. An HTLV-1 ELISA was positive. A chest X-ray revealed diffuse and bilateral alveolar and interstitial infiltrates (Images A and B). A brain CT did not reveal focal lesions. A chest CT revealed diffuse nodular and interstitial hiperdensities with discrete pulmonary cavitations in both lung fields (Images C and D). UPCH Case Editors: Carlos Seas, Course Director / Jorge Nakazaki, Associate Coordinator |
|
Discussion: India ink stain, KOH, and culture showed positive results for Cryptococcus neoformans. The diagnosis of Cryptococcal disease can be suspected through clinical and radiological findings. The confirmatory diagnosis relies on direct microscopy using specific cultures in fungal media, antigen detection, or histopathologic identification. India ink stain is an effective method for diagnosis in advanced HIV patients with a sensitivity of 80%. In non-HIV patients, this decreases to 50% (1). Silver stains allow for the identification of histopathological samples, revealing the typical 5-10 micron-diameter encapsulated yeasts with narrow-based budding. Cryptococcus spp can grow on fungal and bacterial media with a turn-around time of 3-7 days in untreated patients (2). Antigen detection is a rapid and extremely accurate diagnostic method for invasive cryptococcal disease. Cryptococcal antigen (CrAg) detection by latex agglutination has a sensitivity and specificity higher than 90% (3). This test allows titer quantification, which is relevant for monitoring and prognosis. A rapid lateral flow assay (LFA) is a simple test recently introduced to clinical practice with exceedingly good test characteristics (4). Our patient's diagnosis was confirmed after an India ink stain and sputum culture returned positive. Cryptococcal disease causes 250,000 deaths annually, affecting mostly HIV-infected patients. Surprisingly, the mortality attributable to cryptococcosis is higher in non- HIV infected compared to HIV- infected patients (5). Pulmonary disease can range from asymptomatic infection to life-threatening acute respiratory distress syndrome. Radiographic characteristics include lobar radio-opacities, single or multiple non-calcified pulmonary nodules, and cavitary lesions (6). Oral mucosal lesions are exceedingly rare. The cases described have resulted from hematogenous spread from primary lung or CNS infections. The co-existence of pulmonary and oral mucosal lesions should raise suspicion for other infectious agents such as disseminated progressive histoplasmosis, disseminated paracoccidioidomycosis, and for non-infectious etiologies such as non-Hodgkin lymphomas and metastatic squamous cell head and neck carcinomas. HTLV-1 is the first retrovirus described, affecting around 5-10 million people (7). The most common transmission routes are through contaminated blood products and vertically through breastfeeding (8). Most patients remain asymptomatic. A minority can present autoimmune manifestations such as tropical spastic paraparesis (HAM/TSP), malignant complications such as adult T-cell leukemia/lymphoma (ATL), and infectious complications such as crusted scabies, tuberculosis, and strongyloidiasis. The association of HTLV-1 and Cryptococcus spp. has been previously reported. Case reports from Asia and the Caribbean have described mainly pulmonary disease. Interestingly, case reports from Latin America have shown mainly meningeal involvement. (9,10). Disseminated infection was confirmed in our patient after a positive India Ink stain from the oral ulcers was found. Treatment of disseminated cryptococcosis is based on an induction and a consolidation phase. The first-line induction phase includes intravenous liposomal Amphotericin B and 5-flucytosine. A recent African RCT demonstrated non-inferiority in single-dose liposomal Amphotericin B compared to a 14-day standard regimen (11). Although liposomal Amphotericin B has a better safety profile than Amphotericin B deoxycholate, it still has significant adverse effects, particularly renal involvement. A new study has proposed oral Amphotericin B tablets, which could improve adherence and decrease hospitalization time and quality of life (12). These new advances are still to be included in international guidelines. Management of HTLV-1 infection still revolves around symptomatic management, early detection of complications, and prevention of disease transmission. A research group is working on an oral formulation of amphotericin B for leishmaniasis. This could reduce the drug's adverse effects, improve adherence, and ultimately decrease treatment time, hospitalization, and quality of life. The oral formulation of amphotericin B could also be used in the future to treat fungal infections such as cryptococcosis, but more studies are needed. These new advances are still to be included in international guidelines (13). References |