 |
Gorgas Case 2004-02 |
 |
|
The following patient was seen on the 36 bed infectious/tropical disease unit of the Tropical Medicine Institute.

 History: 65-year-old male presents with an indurated, red, infiltrated lesion affecting the entire nose. The lesion began 4 months earlier as a painless red papule on the surface of the left nostril. No nasal discharge, stuffiness, or bleeding. No history of sinus pain, headache, neurologic symptoms, fever, constitutional symptoms, respiratory or intestinal symptoms. No previous medical history. No similar disease in other members of the family. Patient initially treated with a course of antibiotics for cellulitis with no result and then referred to the national cancer hospital where a biopsy ruled out malignancy.
Epidemiology: Born and lives in Cajamarca in the Andean highlands in a rural area (no electricity, no running water and sewage). Works as a farmer. Swims regularly in a river near his house but never in the ocean. No exposure to TB. No travel to the jungle. Physical Examination: Afebrile. Physical findings restricted to the painless, infiltrative and indurated red-violaceous lesion affecting the nose as shown in Image A. No mucosal involvement. Laboratory Examination: Hematocrit 47%, WBC 7200, 55% neutrophils, 29% lymphocytes. Normal glucose, creatinine, urea, and electrolytes. Normal chest x-ray. CT scan of brain and sinuses normal. HIV negative.
|
|
Diagnosis: Balamuthia mandrillaris (free-living amoeba).
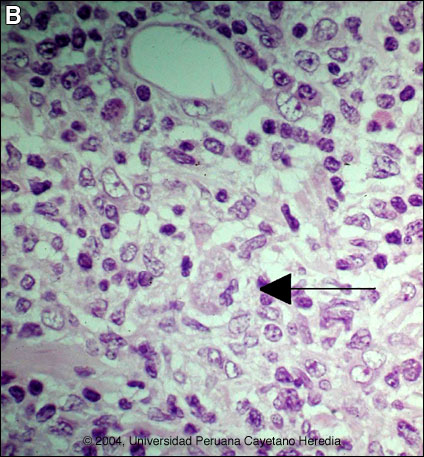
Discussion: The patient underwent a repeat biopsy at our institute. H&E staining shows at the top a capillary and beneath it a dense inflammatory infiltrate composed of mononuclear cells, plasma cells, and lymphocytes. There is a single trophozoite of a free-living amoeba [Image B, arrow]. Note the small red nucleus eccentrically located and the vacuolated cytoplasm. The cells with vacuolated nuclei are endothelial cells, and should not be confused with the parasite. Definitive identification of Balamuthia requires culture or specific immunostaining, which is pending in this case. Other species of free-living amoeba are not known to occur in Perú. Around 100 cases of Balamuthia mandrillaris have been reported since the organism's initial description in 1990 [Clin Infect Dis. 1997 Dec;25(6):1354-8]. Half or so have been in the USA, mostly in immunocompromised patients. Additional reports have come from Canada, Japan, Australia, Thailand, and Eastern Europe, as well as from throughout Latin America. This is the 46th case seen at our institution and, like most Latin American cases, the patient is not immunocompromised. Unlike Acanthamoeba and Naegleria species, which are more familiar to clinicians and known to occur in brackish ponds and creeks, an ecologic niche in nature has not been found for Balamuthia. Our patients have come from throughout rural areas of Perú, and usually, but not always, have a history of swimming in potentially contaminated fresh water. Entry of water into the nasal mucosa and the olfactory nerve endings is thought to occur with Acanthamoeba and Naegleria. Naegleria infection causes an acute necrotizing and suppurative meningoencephalitis, an aggressive disease which is generally fatal in days. Acanthamoeba cause a sub-acute granulomatis encephalitis with a more prolonged but ultimately fatal course. Occasionally patients with Acanthamoeba have a skin lesion usually described as a chronic ulcer. In Balamuthia infection the disease follows a prolonged course but, with rare exception, has a fatal outcome. Almost all cases have an initial skin lesion, and this lesion precedes the inevitable CNS disease by weeks or months. Patients have ranged from 5 to 65 years of age with 50% under age 15. The typical skin lesion is a single painless plaque up to several centimeters in diameter; a few patients have had 2 to 3 lesions. Color may be skin tone, dark red, or slightly violaceous, as in the present patient. Sensation is preserved. Location is usually on the central face but occasionally on trunk or extremities. For facial lesions the differential diagnosis may include tuberculosis, mucocutaneous leishmaniasis, leprosy, sporotrichosis, paracoccidioidomycosis, rhinoscleroma, or mucormycosis. Sarcoid, discoid lupus, and Wegeners can also be considered. Histologically, granulomatous inflammation with lymphocytes, histiocytes, plasma cells, as well as giant cells, is characteristic. Amoebic trophozoites are scanty and multiple sections need to be examined. Some foci of vasculitis may be present. CNS involvement manifests with heachache, photophobia, seizures which progress to lethargy, sensorimotor deficit, coma and death. The CNS lesion is a progressive hemorrhagic necrosis with large numbers of amoebic trophozoites and cysts invading vascular sub-adventitial areas of arteries, veins, and capillaries, leading to perivasculitis and cerebral infarcts [Hum Pathol. 1999 Mar;30(3):269-73]. No therapy has been shown to be highly effective in curing Balamuthia infection. With IV amphotericin B or pentamidine, an initial and apparently favorable response or disappearance of cutaneous lesions still does not halt the eventual appearance of CNS disease. Similarly, in our hands, multi-drug combination therapy with agents such as albendazole, itraconazole, or fluconazole have still resulted in eventual appearance or progression of CNS disease in all but 2 cases. These 2 cases received 6-9 months of albendazole maintenance and were disease free at 3 year follow-up. One or two case reports from other centers have reported success with regimens that have also included sulfadiazine, macrolides and phenothiazines. Based on limited data pentamidine, cotrimoxazole, and phenothiazines can be considered for initial therapy.
|