 |
Gorgas Case 2005-04 |
 |
|
The following patient was seen by course participants in the outpatient department of the Tropical Medicine Institute.

 History: 62-year-old male with a 2 year evolution of skin lesions which began with what he describes as hives on the face and then progressing to involve skin over the entire body. The lesions are non-tender, non-painful, and non-pruritic. No fever, swelling, or systemic symptoms. Mild weight loss.
Epidemiology: Lifelong resident of rural jungle region of Peru. Physical Examination: Afebrile. Erythematous infiltrative plaques, mostly confluent, involving the whole body including palms and soles [Images A, B, C]. These plaques have an ill-defined peripheral margin but a punched out center with well-defined inner margin. Lesions show impairment of sensation most marked in the center (punched out area). He has thickening of the left ulnar, a branch of the left radial (wrist level), both common peroneal and right posterior tibial nerves. There is some loss of motor strength in both ulnar nerves and very mild loss of motor strength in the left radial nerve. There is marked impairment of sensation in the left hand and foot. Laboratory Examination: Hematology and biochemistry unremarkable. A skin biopsy was obtained.
|
|
Diagnosis: Mycobacteria leprae. Multibacillary leprosy according to the WHO classification. Borderline borderline (BB) leprosy according to the Ridley-Jopling classification.
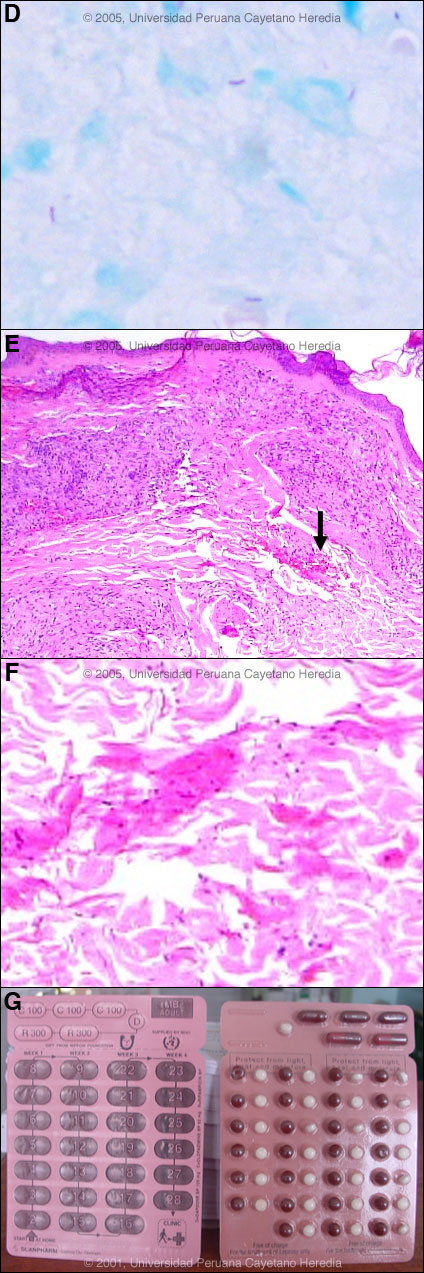
Discussion: With this classic clinical picture and with limited resources, the clinical picture in this patient would provide a definitive diagnosis [reviewed in Lancet. 2004 Apr 10;363(9416):1209-19]. In this patient, we did obtain slit skin smears stained for acid-fast bacilli with the following results: 4+ from the right earlobe, 1+ from the left earlobe, 1+ from the right elbow, 4+ from the left elbow, 3+ from the right knee, 4+ from the left knee and 4+ from one plaque [see Image D]. Slit skin smears are performed by making small (5mm length, 2 mm depth) slits in pinched skin (to avoid bleeding), the edges of which are scraped. The material obtained is smeared on a clean slide and stained for AFB. Generally ear lobes, elbows, and knees are examined. The bacterial index ranges from zero (no bacillli in 100 oil-immersion fields) to 6+ (over 1000 bacilli in one field). A biopsy of a plaque [see Images E, F; arrow shows clusters of acid-fast organisms] showed 3+ acid-fast bacilli consistent with multibacillary leprosy. The usual and most practical grading system is the WHO classification. For therapeutic purposes, it matters only whether the patient has paucibacillary or multibacillary disease. Where no slit skins smears can be done, paucibacillary leprosy is defined as five or fewer skin lesions; multibacillary cases have six or more lesions. Paucibacillary disease usually presents with small numbers of hypopigmented erythematous macules or plaques with absent sensation, well demarcated borders and some scaliness. Multibacillary disease is usually widespread at diagnosis with infiltrated areas of skin with indistinct borders, non-anesthetic papules or nodules. The disease can be classified precisely in the immunologic sense using the traditional Ridley-Jopling classification. This is a spectrum of disease ranging from tuberculoid leprosy (TT) with no or few AFB in lesions and good cell mediated immunity, to lepromatous leprosy (LL) with many AFB and poor cell-mediated immunity. Leprosy is a disease of peripheral nerves and skin. Our patient had clear neuropathy, with marked impairment of sensation on the skin lesions, one foot, one hand, less marked changes on the other hand and foot, and thickened peripheral motor nerves with slight decrease in strength in some. Leprosy can be diagnosed in any patient with simultaneous skin lesions and sensory loss on them unless there is hyperkeratosis. Peripheral nerves such as the ulnar, median, common peroneal, posterior tibial, facial, and greater auricular are often palpably enlarged. In advanced neuropathy this often leads to motor deformities such as claw hand, footdrop, claw toes, and hand and foot insensitivity. The plaque with punched out center is a typical lesion of BB leprosy. Because this type of leprosy in the middle of the spectrum is so unstable, patients tend to move along the spectrum. In this case, because of the widespread and almost complete involvement of all the skin, our patient is probably moving towards the BL (borderline lepromatous) side of the spectrum. The standard WHO regimen for paucibacillary disease is 100mg Dapsone a day unsupervised and 600mg Rifampin once per month directly observed for 6 months. For multibacillary disease patients receive 100mg Dapsone and 50mg Clofazimine a day unsupervised and 600mg Rifampin and 300mg of Clofazimine directly observed once per month. A standard WHO multibacillary dose-pack is shown [Image G]; the instructions in English must be clarified for all healthcare staff and patients. WHO now recommends only 1 year of therapy for multibacillary cases [controversy discussed in Lancet. 2004 Apr 10;363(9416):1209-19], but some would treat those with high bacterial indices (4 to 6+) for the previously recommended 2 years due to higher relapse rates. A myriad of treatment reactions can occur, the possibility of which should be informed and explained to the patient before starting treatment and a reference text should be consulted prior to initiation of therapy by anyone not familiar with these. Response to therapy will be good in this patient. He should increase his cell-mediated immunity against leprosy as we kill the bacilli and he will be cured with no deformities. So-called Type 1 or reversal reactions may occur in up to one-third of borderline patients. These are caused by increases in T-cell reactivity to mycobacterial reactions with infiltration of reactive CD4 cells into skin lesions and nerves. The edema and painful inflammation must be treated urgently with high-dose steroids in order to prevent further nerve damage. After treatment is completed, some patients may recover partially their skin sensation, but longstanding nerve damage is irreversible.
|