| 2006 Case #4 |  |
|
| The following patient was seen on the 36-bed tropical disease unit of the 450-bed Cayetano Heredia National Hospital. |
 History: 16 yo male admitted after a 20-minute episode of headache followed by tonic-clonic movements of the right arm with subsequent generalized seizure and loss of consciousness. Several similar episodes occurred while he was 2 to 5 years old. History: 16 yo male admitted after a 20-minute episode of headache followed by tonic-clonic movements of the right arm with subsequent generalized seizure and loss of consciousness. Several similar episodes occurred while he was 2 to 5 years old.
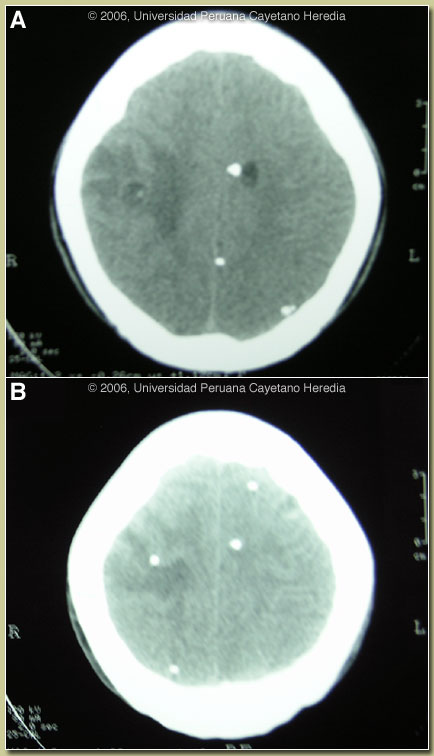
Epidemiology: Born in Jauja-Junin (highlands). Pig farmer now living in Lima. No TB exposure or history. Physical Examination: Afebrile, respiratory rate 16, BP 100/60. Normal physical and neurological exam including fundoscopy. Laboratory Examination: Hct 37%, WBC 8500 with normal differential (0 eosinophils). Glucose, electrolyes normal. Chest X ray: normal. CT-scan without contrast is shown in Images A and B.
|
Cysticercosis is infection with the larval stages of the human pork tapeworm Taenia solium. Humans acquire cysticercosis after ingesting eggs of T. solium in material contaminated with feces originating in human tapeworm carriers. Humans that do not eat pork can get cysticercosis. Ingestion of contaminated pork results in humans getting an adult intestinal tapeworm not cysticercosis. Cysticercosis is common in many developing countries and very common in rural agricultural areas of Peru. In developed countries the long-lived cysticerci are increasingly seen as immigration from affected areas rises. Occasional transmission by tapeworm carriers to those who have never left non-endemic countries is reported.
Ingested T. solium eggs hatch in the stomach and are then carried to the muscles and other tissues where the larvae encyst and reach their usual size of about 1 cm within a few months. Clinical manifestations depend on the affected organ but neurocysticercosis causes the most morbidity. The cysticerci seem able to evade the immune system and are thought to remain viable for several years without causing any inflammatory response. Most clinical symptoms are the direct result of inflammatory responses that accompany the eventual cyst degeneration. Epileptic seizures are the primary or sole clinical manifestation in up to 80% of patients. In endemic regions new onset seizures in teenagers or young adults is most likely due to neurocysticercosis. Cysticerci can also cause symptoms because of mass effect, impingement on a vital structure, or blockage of CSF circulation especially if the cyst is intraventricular.
Seizures need to be managed as per any other form of epilepsy. Treatment of parenchymal neurocysticercosis with antiparasitic drugs is highly controversial. Albendazole clearly kills the cysts, but many believe that since the cysts only cause symptoms when they are dying anyway, the use of antiparasitic drugs may lead to unnecessary added inflammation and exacerbation of symptoms. Placebo-controlled trials are few and conclusions difficult because there are many types and magnitudes of disease [see review Lancet. 2003 Aug 16;362(9383):547-56]. A panel of experts has published consensus recommendations for some clinical presentations and identified areas of continued disagreement [Clin Microbiol Rev. 2002 Oct;15(4):747-56]. Therapeutic decisions should be based on the number, location, and viability of the cysts. Patients in whom all lesions are already calcified should receive no anti-parasitic treatment. Patients with moderate disease with more than 5 viable lesions (even in the presence of other calcified lesions) should receive therapy with albendazole under steroid cover. There is continued disagreement over patients with only one or a few viable cysts such as our patient (treatment may be unnecessary), patients with only degenerating cysts (treatment may be unnecessary), and patients with massive infections with viable cysts (high risk of much cerebral edema). Separate considerations apply to patients with subarachnoid, ventricular, or intramedullary disease and are not discussed here.
Our patient with at least 3 viable lesions desired treatment. Since calcified scars may result in chronic epileptogenic foci, the main issue is whether treatment or natural evolution of the dying cyst leads to better long-term outcomes with respect to seizure control. Our patient was referred for entry into an ongoing randomized blinded trial comparing 28 days of steroids (8mg/d of dexamethasone) to the standard 6mg/d for 10 days in controlling seizures. Albendazole for 10 days is given openly to all patients as well as antiseizure medications.
{/slide}