 |
Gorgas Case 2008-02 |
 |
|
The following patient was seen in the inpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital.
 History: 31-year-old male with a four-month history of progressively worse cough with onset of left pleuritic chest pain one month into the illness. No fever or weight loss but some scanty sputum. Antibiotics led to no improvement. An acute deterioration occurred one day prior to admission and the cough became more severe with production of large amounts of liquid sour tasting salty sputum. He developed progressive dyspnea severe enough to take him acutely to the emergency room where he was also complaining of acute pruritus.
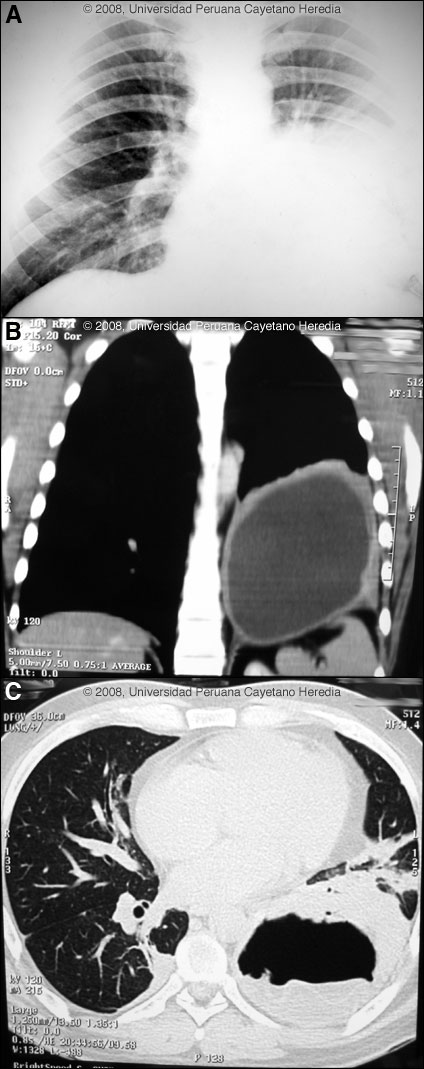
Epidemiology: The patient is a lifelong resident of the Andean highlands around Abancay. He is an anthropologist who travels extensively across the country. No history of or known exposure to TB. No ingestion of uncooked food. Physical Examination: Afebrile, respiratory rate 29, pulse: 100, BP: 100/60. Decreased breath sounds with dullness in the left lower lung, diffuse rhonchi with wheezing. No hepatosplenomegaly. A diffuse erythematous rash was present diffusely. Laboratory Examination: Chest X-ray 1 week prior to acute deterioration [Image A] and computer reconstructed view [Image B] from a CT scan performed at the same time. A CT scan just after admission is shown in Image C. Hematocrit: 44%, WBC: 17,000 (94 neutrophils, 1 eosinophils, 1 basofils, 2 monos, 4 lymphs), 317,000 platelets. Sputum AFB negative. Normal liver function tests and abdominal ultrasound was normal. A diagnostic procedure was performed.
|
|
Diagnosis:Echinococcus granulosus. Acute rupture of hydatid cyst into a main bronchus.
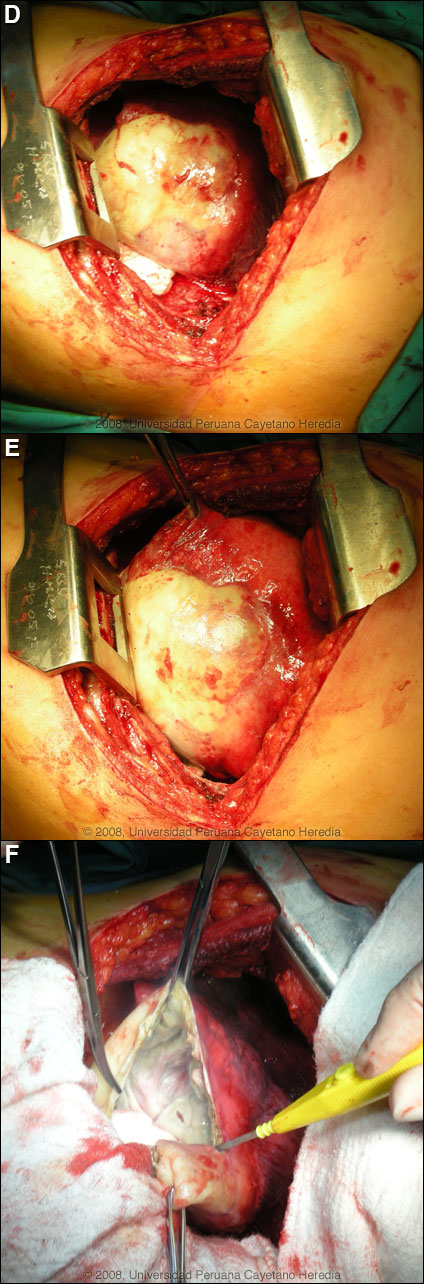
Discussion: A Western Blot taken before the acute rupture was strongly positive for E. granulosus. The expectoration of large amounts of salty fluid is highly characteristic of this catastrophic event. The 2nd CT scan showed no pleural fluid indicating erosion and rupture of the cyst only into the bronchus. The elevated peripheral WBC is likely indicative of some bacterial superinfection post-rupture. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. Sheep are the normal intermediate hosts. Larval cysts expand slowly over years or decades becoming symptomatic as they impinge on other structures by virtue of their size. Spontaneous cyst rupture as occurred here happens in the minority of cases but is not rare. The cysts contain hundreds of viable scoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new scoleces on an ongoing basis. Each scolex is capable of becoming a new daughter cyst either within the original cyst or elsewhere should the original cyst rupture or be ruptured. An example of seeding of the pleural cavity is seen in a previous case of the week (Gorgas Case 2005-10). Hydatid disease is common in sheep-raising areas worldwide. Most primary infections involve a single cyst. 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 15% will also have a hepatic cyst. Serology is usually positive with hepatic cysts but sensitivity drops below 50% with solitary pulmonary cysts even when the cyst is large. With the large burden of disease in this patient’s lung a positive serology would be expected. Praziquantel is the most potent scolicidal drug and is the drug of choice for all adult tapeworms. However, praziquantel cannot penetrate the hydatid cyst wall so is only useful as an acute therapy when a cyst ruptures (spontaneously or due to surgical mishap) and scoleces are lying free before encysting again. Albendazole is the therapy of choice for intact cysts that are not operable, such as when there are multiple or diseminated cysts. A trial of Albendazole may also be considered for solitary cysts that are less than about 10 cm. Response is generally slow and only complete in a minority of cases. Surgical resection is the therapy of choice for large intact solitary cysts and certainly in a case like this with an acute rupture and a broncial-cyst fistula. At thoracotomy, the cyst was found to be intact on all surfaces within the lung parenchyma and was flaccid with little remaining fluid indicating that fortunately no fluid (which would contain protoscoleces) [Images D, E] had escaped into the pleural space. Unfortunately, the outer membranes were highly adherent to the lung parenchyma precluding shelling out and removal of the cyst alone and necessitating a left lower lobectomy. Image F shows the inner or germinal membrane that lines the cyst and that is responsible for the ongoing generation of new protoscoleces as the cyst grows in size. Perioperative Albendazole in case of cyst rupture during the procedure is frequently utilized for hepatic cysts even though scolididal agents are always injected into the cyst intraoperatively before any resection is attempted. In the case of pulmonary cysts most surgeons feel that cyst softening that may occur with albendazole makes the operative procedure more complicated and increases the risk of rupture at the time of resection.
|