 |
Gorgas Case 2008-03 |
 |
|
The following patient was seen in the inpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital. We would like to thank the attending physician Dr. Ciro Maguiña for advice and also thank Gorgas Course Visiting Professor David Warrell from Oxford University, who is with us in Lima this week, for perspectives on other similar cases.
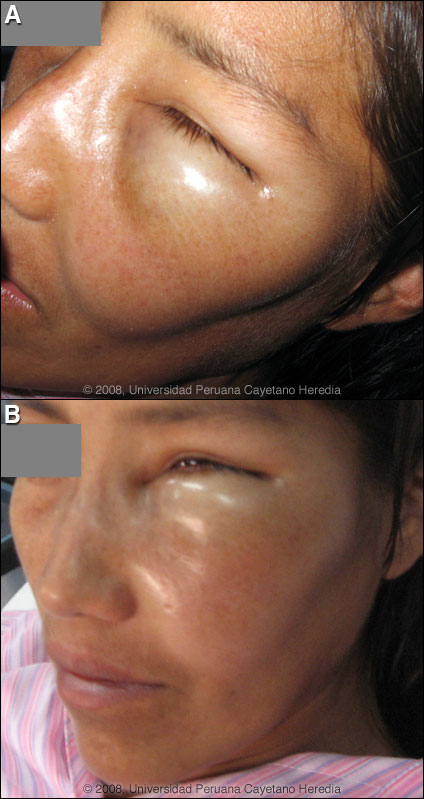
 History: 30 yo female with acute onset of local pain and facial edema. She had been awakened at 1:00 am by a burning sensation in the left peri-orbital region. Five hours later the lesion had become swollen and warm and acutely painful. No headache, nausea, vomiting, impaired eye movement, blurred vision or fever. No history of trauma, no recent sinusitis. No past medical history, no current medications. Epidemiology: Housewife, born in Piura (northern Perú) but currently living in Puente de Piedra, Lima in a pre-fabricated house with running water, sewage and electricity. Physical Examination (11:00 am next morning): Afebrile, normotensive, HR 72. Pain and marked edema left periorbital region [Images A, B]. No proptosis. Ocular fundus clear with normal extraocular movements. Laboratory Examination: Hematocrit 36, WBC 7350 (73 neutrophils, 1 eosinophil, 5 monocytes, 21 lymphs), Platelets: 220 000, INR: 1.08; liver function tests, glucose, creatinine and CK were normal. Normal urinalysis.
|
|
Diagnosis: Necrotic araneism due to bite of the South American brown recluse spider Loxosceles laeta [Image C].

Discussion: The diagnosis of loxoscelism is a clinical one though definitive criteria for the diagnosis require knowledgeable species identification of the offending spider. In this case, the patient had seen and crushed a brown spider (not brought to the hospital for examination) on her face at the time of the onset of symptoms. L. laeta are highly prevalent in Puente de Piedra, Lima the exact area of this patient’s residence. The spectrum of disease ranges from a mild skin irritation, to severe local necrotic reactions, to a less common syndrome (10-15% of cases) of viscerocutaneous loxoscelism manifested with dramatic fever, blanching, dengue-like scarlatiniform rash, hemolysis and renal failure. Mortality may uncommonly occur in severe cases and is higher in children due to lower body weight per amount of venom injected. The classic “red white and blue” sign [Image D, another patient from the Gorgas archives] is virtually diagnostic as the lesion evolves. The erythematous outer ring is vasodilatation, the middle white ring is vasoconstriction, the central blue is pre-necrotic cyanosis. This pattern was noted in our patient on Day 3 [Image E]. The initial bite is often noted by the patient, but it often takes several hours for the onset of severe pain as the venom spreads. The violaceous central plaque represents an area of hemorrhage and thrombosis which in more severe cases will progress to frank necrosis. The bite of Loxosceles laeta is thought to cause more extensive and severe necrosis when compared to the related and well-studied brown recluse spider Loxosceles reclusa found in the United States. When the lesions do evolve there is a hemorrhagic bulla, ulceration, and development of necrotic centers. The borders are irregular, influenced by gravitational factors as venom spreads in a manner related to the body part affected and without the significant surrounding edema. Our patient received 2 vials of polyclonal equine IV antiserum produced by the INS-Perú 15 hours after the bite. She also received analgesia, dapsone (100 mg/d) for 7 days plus oral clindamycin. Evolution of the lesion is shown at Day 7 [Image F], and Day 9 [Image G]. Surgical scar revision will be performed. Work in animal models has shown anti-venom to be effective if administered in the first 12-24 hours after a bite, but prospective controlled human clinical trials are lacking in any country [Toxicon. 2006 Aug;48(2):123-37]. Retrospective data is limited by lack of definition of time to antivenom adminstration and relation of that parameter to outcome. There is no commercial product available in North America. In Perú a polyvalent equine antiserum raised against Loxosceles laeta and Loxosceles rufipes is produced by the INS-Perú and a Brazilian equine preparation is widely used in that country. It is administered intravenously once, 10 ml for adults and 5 ml for children. In Perú, as in many other countries that have various Loxosceles sp., dapsone is administered at 100 mg/day for 1 week unless patients already have active hemolysis or are G6PD deficient. No controlled trials have been reported, the practice is controversial, but clinical experience in Perú and several limited studies support this practice. G6PD deficiency does not occur in Perú. Systemic corticosteroids are often considered but again, no clinical trials support the practice. Patients with any evidence of hemolysis or hemoglobinuria require vigorous intravenous hydration and urinary alkalinization. Aggressive debridement and escharectomy is usually advised once the acute phase is over but too early debridement may increase tissue loss. At least 54 species of Loxosceles are described from North and Central America, 30 from South America, and additional species are found in Africa and the Mediterranean. Loxosceles laeta is native to Perú, Chile, Ecuador, Argentina, Uruguay, and south and eastern Brazil. It has been accidentally introduced into the U.S. and several Central American countries at various times but does not naturally thrive in those locations. Loxosceles laeta is similar in appearance to other recluse spiders but is generally larger with a body length up to 15 mm [Image C]. The head region has dark violin shaped markings on the dorsal aspect [see inset in image C] but these markings cannot be reliably used to identify recluses as other types of spiders may have similar markings. Loxosceles laeta accounts for 98% of loxosceles cases in Perú, but is only seen in coastal regions and up to 1200 m in the Andes but never in the jungle regions. However, jungle species such as L. amazonica may be found in Brazil. They live most commonly in very domestic environments in both urban and rural areas, often hiding in clothing in drawers or in closets. They are not aggressive and only bite when disturbed or threatened. Bites occur more commonly in summer (January-April) when the spider reproduces and most bites occur at night or in the early morning.
|