| 2008 Case #4 |  |
|
| The following inpatient was seen by the Gorgas Course participants. We would like to thank Dr. Carlos Seas, Gorgas Course Clinical Coordinator. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
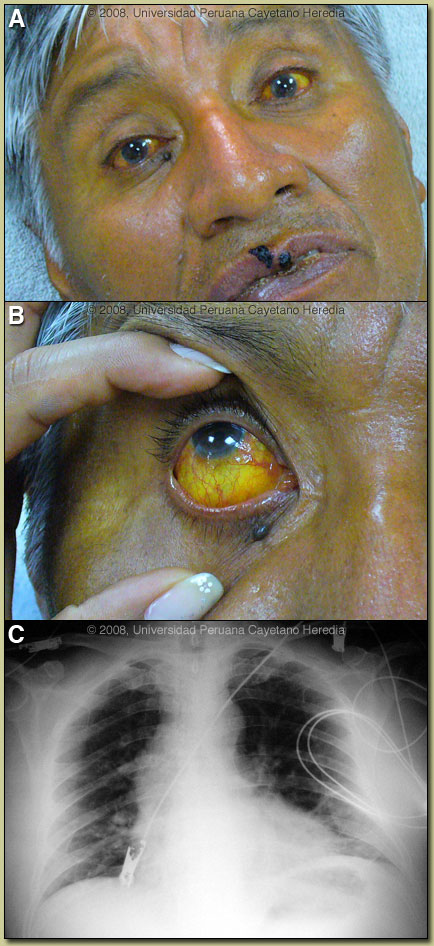
Epidemiology: Office worker and lifelong resident of Lima. He had been on vacation in Supe on the coast north of Lima for 10 days and became ill there. No other recent travel. No history of bathing or swimming in lakes, ponds, rivers or water channel but he swam in a public pool which uses underground water without chlorine. In Supe all water is stored in a tank at the house where he stayed. Past medical history is non-contributory. Physical Examination: BP 120/70, Temperature 38.5°C, pulse 100, respiratory rate 22. Acutely ill patient with marked jaundice apparent in both skin and eyes [see Image A & B]. No rash, no lymphadenopathy, scattered rales bilaterally, liver palpated 4 cm below the right costal margin, spleen tip was palpable. Normal neurologic examination. Laboratory Examination:
Three blood films negative for Bartonella and malaria. Two blood cultures and one bone marrow culture negative. Negative slide agglutination tests for Salmonella and Brucella. Dengue IgM ELISA negative. Chest x-ray shows alveolar infiltrates and some atelectasis at the right base [Image C]. Abdominal ultrasound showed mild non-focal hepatomegaly and mild splenomegaly. |
| Diagnosis: Leptospirosis. |
| Discussion: Serology by the Microagglutination technique (MAT) was positive for Leptospira interrogans serovar Coppenhageni at 1/1600 on a convalescent specimen taken one week after the acute specimen which had been 1/400 on day 10 of illness. Cutoff for a single positive test is 1/200.
Leptospirosis needs to be considered in the differential diagnosis of any undifferentiated tropical fever. It has protean clinical manifestations and at differing stages of the illness may be impossible to distinguish clinically from yellow fever, dengue, rickettsial disease, typhoid, malaria, brucellosis, tuberculosis, viral hepatitis. The clinical course here is too long for dengue or yellow fever. Patients with viral hepatitis become afebrile with the onset of jaundice. Typically, leptospirosis is described as having an initial septicemic phase which may be mild, with fever, myalgia, headache, conjunctival suffusion, and abdominal wall pain. Our patient had the conjunctival suffusion and the muscle tenderness in calves and lumber areas often described as distinguishing features of leptospirosis. The illness may be self-limited but in some cases, after an apparent recovery, may present a biphasic illness and progress to an immune stage manifest by fever, meningitis, and uveitis. As in this case, the two distinct stages may be obscured and run together in severe disease (Weil’s Disease) manifested by the classic defining triad of jaundice, hemorrhage, and renal failure. Weil´s disease has a mortality of 10%. A separate entity, severe pulmonary hemorrhage syndrome presents with hemoptysis, resipiratory insuffiency, and has a mortality of 50%. Altered mental status was found to be the strongest predictor of death in two studies yet a specific central nervous system process has not been identified which can explain this finding. The classically described textbook manifestations of leptospirosis represent only a small portion of a much wider spectrum of disease. In Iquitos in the Peruvian jungle, as in many other areas of the tropics, data indicates a seroprevalance of up to 40% of the general population, with most individuals not having a discernible history of a prolonged febrile illness consistent with typical descriptions of leptospirosis [Lancet Infect Dis. 2003;3(12):757-71]. This is consistent with the feeling that most cases in the tropics are not diagnosed due to the non-specificity of the illness and the inavailablity of diagnostic tests in resource poor environments. Jaundice and bilirubinemia out of proportion with hepatocellular damage is the usual finding in leptospirosis. This is manifest as significant jaundice in the face of an SGOT and SGPT that is no more than 3-4X normal with an alkaline phosphatase that may be as high as 10X normal. The mechanism of the cholestasis in leptospirosis is not entirely clear. In severe or prolonged disease, renal damage will occur and the sediment is usually active. Non-oliguric hypokalemic renal failure as found in this case is characteristic. Progression to oliguric renal failure is predictive of higher mortality. Isolation of Leptospira in culture is difficult and insensitive. Culture in special media in tubes held at 28-30°C for prolonged periods is necessary. Blood is only positive in the first week of illness after which urine becomes progressively more positive. Cultured leptospires are only visible and confirmed using dark-field microscopy. Diagnosis is most often serological and retrospective [MAT], IgM ELISA, or a commercially available rapid dipstick test. PCR-based diagnosis is effective, quantitative, and rapid compared to other techniques but remains a research tool. Patients with severe disease usually have >10,000 organisms per ml of blood or tissue. Leptospirosis is endemic in almost every country but more so in the tropics. Traditionally an occupational disease and a disease of poverty in peri-urban slums, it has also emerged as a disease of adventure travelers (hikers, bikers, boaters, swimmers) who have contact with standing or moving water. Leptospires may penetrate conjunctiva, macerated skin, or possibly the oropharynx. Leptospirosis is maintained in the environment by long-term carriage and excretion of the organism from the urinary system of asymptomatic animal carriers. Rodents are most frequently implicated with swine, cattle, and dogs next most frequent, but the full spectrum of mammals forming the reservoir is unclear. Classification of leptospires is complex and obscure to most clinicians. While most human isolates are L. interrogans, further division into a number of species using DNA relatedness is hampered by a traditional naming system that uses serologically defined antigenic determinants (serovars and serogroups) that may be shared by two or more species. Recent trials support the use of intravenous antibiotics for severe disease. Cefotaxime or ceftriaxone are equivalent to penicillin and much more convenient due to once daily dosing [Clin Infect Dis. 2003;36(12):1507-13, Clin Infect Dis. 2004;39(10):1417-24]. Milder disease may be treated with oral doxycycline. Efficacy appears best when treatment is begun within 4 days of illness onset. Our patient was treated with IV ceftriaxone (2gm/d the first day followed by 1gm/d for 10 days); muscle pain resolved after four days, fever subsided after three days but the jaundice has persisted for longer. Doxycycline 200 mg po once per week has been shown to prevent disease in high-risk individuals such as military personnel on maneuvers and adventure travelers.
|