| 2008 Case #8 |  |
|
| The following patient was seen in the outpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital in Lima, Perú. We would like to thank the Gorgas Course Dermatology Professor Dr. Francisco Bravo. |
|
Epidemiology: The patient was born in and is a lifelong resident of Lima. His parents migrated from Ayacucho in the Andean Highlands. Physical Examination: Afebrile. Diffuse erythema and scaling with evidence of lichenification over the trunk and limbs [Images A & B]. Marked hyperkeratosis of the dorsum of hands and web spaces [Image C]. No mucosal involvement. Exam otherwise unremarkable. Laboratory Examination: No basic CBC or biochemistry obtained. |
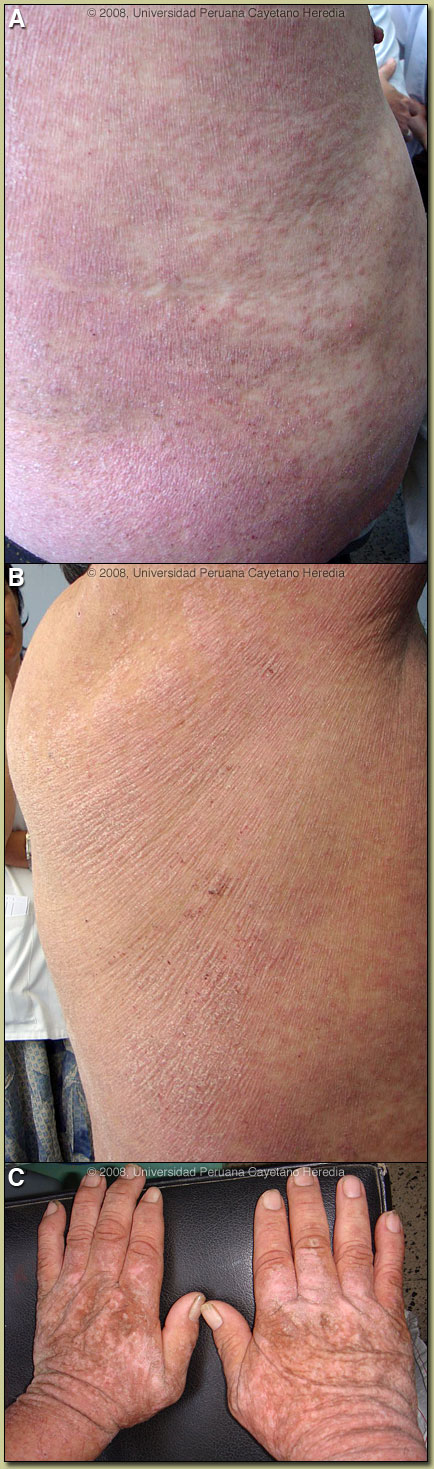
| Diagnosis: Crusted scabies (also called Norwegian scabies). HTLV-1 infection. |
| Discussion: Skin scrapings viewed by direct microscopy disclosed 2-3 Sarcoptes scabei per each high power field, a remarkable density. ELISA and Western blot for HTLV-1 were both positive in the patient. Two sisters of the patient have also tested positive for HTLV-1 and one of them has tropical spastic paraparesis [see Gorgas Case 2002-08]. All 3 siblings were breastfed for prolonged periods. The mother is no longer alive.
The crusted diffuse highly pruritic skin lesions in this patient are very characteristic for Norwegian scabies. This condition is well-described in many immunocompromising conditions including HIV infection, malignancy, and immunosuppressive therapy. The skin is hyperinfested with thousands of mites, so it is easily diagnosable with simple scrapings. The lesions are highly infectious and present a serious nosocomial risk. At the Tropical Medicine Institute in Lima approximately 70% of all cases of Norwegian scabies are associated with HTLV-1 infection and are, in the absence of any other factors, associated with immunosuppression. Other opportunists associated with HTLV-1 are strongyloides infection (negative Baermann stool concentration in our patient), onychomycosis, and acute infectious dermatitis of childhood [see Gorgas Case 2004-07]. Similar to HIV, several recent cross-sectional studies have found a high prevalence of HTLV-1 among tuberculosis patients and a high prevalence of tuberculosis among HTLV-1-infected people. TB mortality may be increased in the face of HTLV-1 infection. Other conditions associated with HTLV-1 infection [see Lancet Infect Dis. 2007 Apr;7(4):266-81 for a detailed discussion] are acute T-cell leukemia/lymphoma and autoimmune disease including tropical spastic paraparesis, Sjogrens, arthropathy, polymyositis, and thyroiditis. This patient did not have any neurological findings. The prevalence of HTLV-1 in South America is generally underappreciated, normally being associated with Japanese and Caribbean populations. HTLV-1 is now known to occur worldwide, having originated in Africa. The highest prevalence is in Japan. In Perú, the disease is highly endemic (2-3% seropositivity) in Andean areas of the country, in Quechua populations who have had no contact with Japanese immigrants to the country. Other South American countries with significant rates of HTLV-1 include Brazil, Colombia, and Ecuador. Transmission appears to be mainly vertical with high associations with breastfeeding and duration of breastfeeding (probable route in our patient). Transfusion, sexual transmission, and IV drug abuse are much less important. Norwegian scabies is not responsive to normal topical agents such as benzyl benzoate or permethrin. Our patient was treated with ivermectin 200 µg/kg bid for 2 days which was repeated 15 days later. The lesions responded dramatically to therapy. Most individuals with HTLV-1 infection remain asymptomatic for life. For those with complications there are few treatment options for the underlying HTLV-1 infection. Trials with anti-retroviral agents and immunomodulators have been uniformly unsuccessful. |