| 2008 Case #5 |  |
|
| This past week, the field trip to Cusco in the Andean highlands took place. Cusco (elevation 3400 m) is the oldest continuously inhabited city in the Americas. This patient was seen on the medical ward of the Regional Hospital of Cusco. We thank Dr. Miguel Villanueva, UPCH Infectious Disease fellow for his help and advice with this case, and Dr. Hector Hugo-Garcia, ___ Unit, Instituto de Ciencias ___, Lima for his advice on the management of this case. |
|
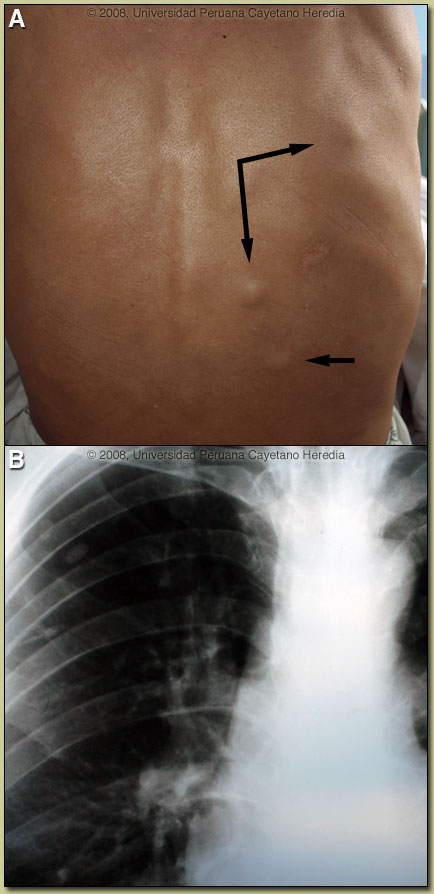
Epidemiology: Born and lives in the highlands near Cusco. Farmer who raises cows, pigs, and guinea pigs. Has dogs and cats at home. No known TB exposure. Moderate alcohol intake. No similar illness in contacts. Physical Examination: BP 110/80. Temp 37.1°C. Cardiopulmonary and abdominal examination normal. Skin: 1 cm non-fixed, non-tender, soft nodules on the abdomen (4), back (5) [see Image A], right thigh (2), inguinal region (1). Neurological: no papilledema, normal cranial nervers, loss of sensation over left leg only. Laboratory Examination: Hematocrit 52% (normal for altitude of 3400 metres). WBC 12.8 (84 segs, 3 bands, 9 lymphs, 4 monos). Glucose 88, normal renal function, normal liver function. Chest x-ray: several calcified lesions seen [Image B].
|
| Diagnosis: Neurocysticercosis due to Taenia solium. Cysticerci in soft tissue. |
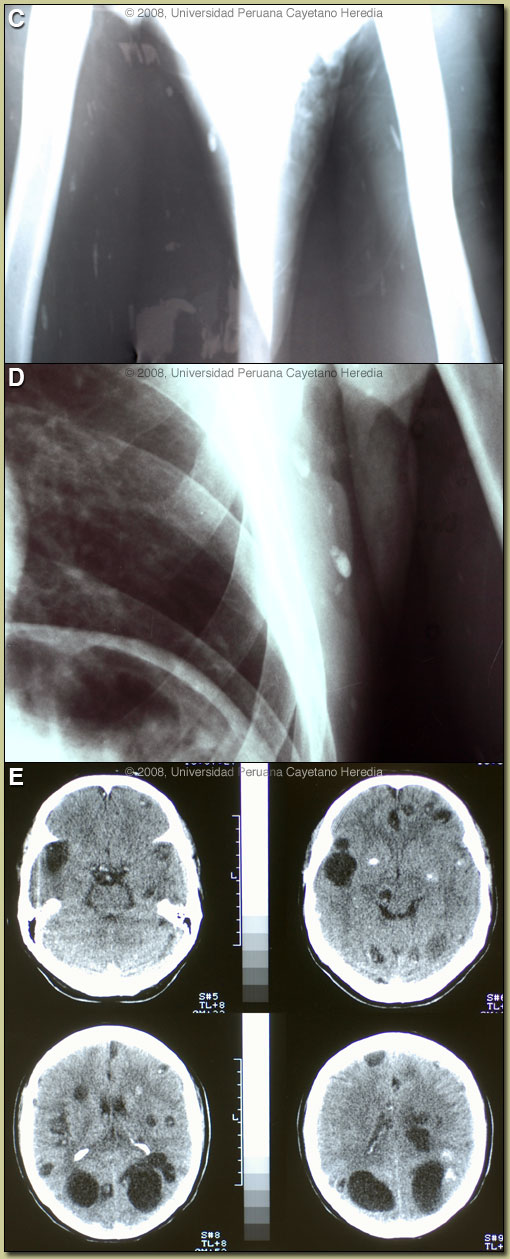 Discussion: X-ray examination of the lower extremities [Image C] disclosed multiple linear cigar-shaped soft-tissue calcifications that are diagnostic of cysticercosis. The calcified cysticercus produces single (rarely) or multiple (often several hundred) calcifications in the soft tissues, which are linear or oval in shape and usually measure 4-10 mm or more in length and 2-5 mm in width. Cysts as large as 23 mm have been reported. The calcified cysts will have their long axes in the plane of the surrounding muscle bundle. No other organism results in a calcification pattern like this. On further review of the Chest X-ray all the calcifications were found to be extra-thoracic and in the soft tissues [Image D]. Discussion: X-ray examination of the lower extremities [Image C] disclosed multiple linear cigar-shaped soft-tissue calcifications that are diagnostic of cysticercosis. The calcified cysticercus produces single (rarely) or multiple (often several hundred) calcifications in the soft tissues, which are linear or oval in shape and usually measure 4-10 mm or more in length and 2-5 mm in width. Cysts as large as 23 mm have been reported. The calcified cysts will have their long axes in the plane of the surrounding muscle bundle. No other organism results in a calcification pattern like this. On further review of the Chest X-ray all the calcifications were found to be extra-thoracic and in the soft tissues [Image D].
A CT scan of the head [Image E] showed a total of 35 lesions in different stages of evolution, including calcified lesions as well as several very large lesions that are bigger than the typical 1-2 cm lesions associated with viable cysts. In this case, these large cysts are (or at least act as) parenchymal cysts. With some frequency cysts in the Sylvian fissure (those which become very large) are actually subarachnoid in nature but behave as parenchymal: seizures, some mass effect with minimal CSF inflammation and usually respond to antiparasitic drugs. Other examples of such large lesions may be found at [http://tmcr.usuhs.mil/tmcr/chapter7/clinical7.htm]. No intraventricular lesions or signs of intracranial hypertension were seen in this patient. Edema around a dying cyst is often the trigger for onset of seizures in infected individuals. Cysticercosis is infection with the larval stages of the human pork tapeworm Taenia solium. Humans acquire cysticercosis after ingesting eggs of T. solium in material contaminated with feces originating in human tapeworm carriers. Humans that do not eat pork can get cysticercosis. Ingestion of contaminated pork results in humans getting an adult intestinal tapeworm not cysticercosis. Cysticercosis is common in many developing countries and very common in rural agricultural areas of Perú. In developed countries the long-lived cysticerci are increasingly seen as immigration from affected areas rises. Occasional transmission by tapeworm carriers to those who have never left non-endemic countries is reported. Ingested T. solium eggs hatch in the stomach and are then carried to the muscles and other tissues where the larvae encyst and reach their usual size of about 1 cm within a few months. Clinical manifestations depend on the affected organ but neurocysticercosis causes the most morbidity. The cysticerci seem able to evade the immune system and are thought to remain viable for several years without causing any inflammatory response. Most clinical symptoms are the direct result of inflammatory responses that accompany the eventual cyst degeneration. Epileptic seizures are the primary or sole clinical manifestation in up to 80% of patients. In endemic regions new onset seizures in teenagers or young adults is most likely due to neurocysticercosis. Cysticerci can also cause symptoms because of mass effect, impingement on a vital structure, or blockage of CSF circulation especially if the cyst is intraventricular. In all cysticercosis patients, seizures need to be managed as per any other form of epilepsy. Treatment of parenchymal neurocysticercosis with antiparasitic drugs such as albendazole is increasingly accepted even when there are few lesions. Albendazole clearly kills the cysts, but may lead to added inflammation and exacerbation of symptoms, which is usually dealt with by empiric concomitant use of steroids. Therapeutic decisions should be based on the number, location, and viability of the cysts. Patients in whom all lesions are already calcified should receive no anti-parasitic treatment. Recent work indicates that long-standing calcified lesions can sometimes provoke peri-lesional edema, which may need treatment with steroids as well as anti-seizure medication. Special considerations apply to patients such as this with large numbers of active lesions due to the chance to induce a diffuse encephalitis due to the severe inflammation due to simultaneous killing of many organisms. Intraventricular shunting may be necessary if intracranial hypertension results from treatment. Neurocysticercosis is a variable disease and treatment approaches need to be individualized to a large number of differing clinical presentations [Neurology. 2006 Oct 10;67(7):1120-7]. Our patient elected treatment with prolonged albendazole for 30 days under steroid cover and anti-seizure medication. In our experience (no controlled data) large cysts do better with treatment longer than the standard 8 days. He has tolerated the first 10 days of therapy without incident and the subcutaneous nodules have shrunk in size. Steroid management in these cases (when you have to maintain it for a long time) is a problem. The idea is to try to decrease doses as soon as possible after the second week of treatment realizing that the attempt may not be immediately successful.
|