Gorgas Case 2008-10 |
 |
|
The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Perú. Each August we run one of our 2-week refresher courses for those with previous training in tropical medicine; currently running is the Gorgas Expert Course. For the past 8 years, we have been pleased to share interesting cases seen by the participants during the weeks of the year one of our courses is in session; there will be one more case next week to complete the 2008 case series. Each case includes a brief history and digital images pertinent to the case. A link to the actual diagnosis and a brief discussion follow. |
| The patient was seen in the surgical ward of the 400-bed Cayetano Heredia National Hospital. |
|
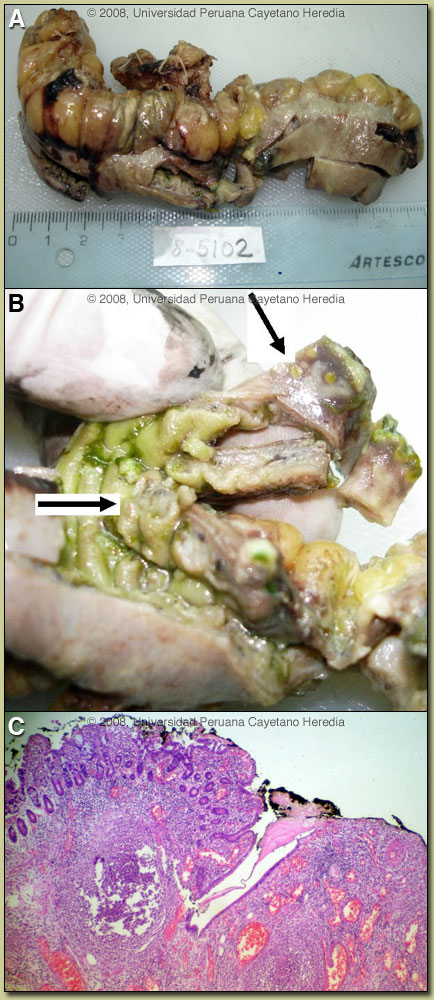
Epidemiology: Born in and lifelong resident of Lima, unemployed, no history of travel. Physical Examination: Temp 37.8°C, pulse 110, respirations 36, BP 100/60. Acutely ill and dehydrated. No lymphadenopathy, no rash. Chest: rales at right base. Abdomen: few bowel sounds, peritoneal signs (rebound tenderness, positive Mc Burney). Normal rectal examination. Laboratory Examination: Hemoglobin 8.6 g/dl, WBC 6000 (2% bands, 84% neutrophils, 10% lymphs), 360K platelets. Glucose 80 mg/dl, creatinine 1.2 mg/dl, hyponatremia (Na 128 meq/l), hypoalbuminemia (total proteins 4.8, albumin 2.0), normal ALT. An urgent laparotomy was performed on admission. A single perforation (0.5 cm in diameter) located in the terminal ileum, 100 cm away from the ileocecal valve, was found [Images A, B]. Multiple enlarged mesenteric lymph nodes were also found. Approximately 1 litre of pus was drained. Histology from surgical specimen is shown in Image C. |
| Diagnosis: Intestinal perforation due to M. Tuberculosis. HIV infection. |
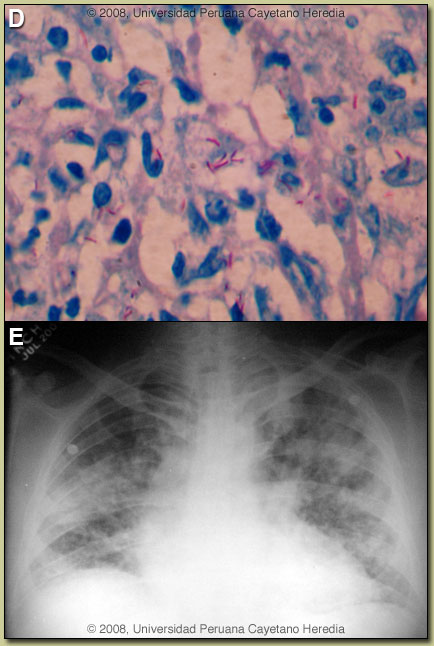 Discussion: Image B demonstrates a single ulcer located in the non-mesenteric border of the ileum with necrotic borders partially covered by fibrin. Microscopy [Image C] demonstrates a perforated intestinal ulcer surrounded by acute and chronic inflammation and epithelioid cells, with no well-formed granulomas. Examination of lymph nodes showed a necrotizing suppurative adenitis also without granuloma formation. Ziehl Nielsen stain of the intestine and lymph node were highly positive [Image D]. Sputum is Z-N positive. Discussion: Image B demonstrates a single ulcer located in the non-mesenteric border of the ileum with necrotic borders partially covered by fibrin. Microscopy [Image C] demonstrates a perforated intestinal ulcer surrounded by acute and chronic inflammation and epithelioid cells, with no well-formed granulomas. Examination of lymph nodes showed a necrotizing suppurative adenitis also without granuloma formation. Ziehl Nielsen stain of the intestine and lymph node were highly positive [Image D]. Sputum is Z-N positive.
On further enquiry one of his sons is currently being treated for smear positive pulmonary TB. The patients chest X-ray is shown [Image E] demonstrating a miliary pattern with bilateral alveolar infiltrates. HIV ELISA is positive; the patient had not previously been tested. In Perú, the main differential diagnosis in a patient with this initial clinical presentation (without knowledge of the chest X-ray findings) would be typhoid fever due to Salmonella typhi complicated by intestinal perforation. Involved Peyer’s patches are generally in the terminal ileum within 60 cm of the ileo-cecal junction and in the cecum itself. Without treatment, after about 7-10 days of illness, necrosis and sloughing of the overlying mucosa may result with ulcer formation and more rarely intestinal perforation. Ulcers are usually 1 cm or less in size and most often solitary. Intestinal perforation due to E. histolytica would usually be preceded by a hemorrhagic colitis and perforation due to Balantidium coli by profuse watery diarrhea [see Gorgas Case 2002-07]. Prevalence data for intestinal TB are sparse either in HIV positive or negative patients but in 1 referral center in Hong Kong it was ~0.5% of presenting cases [see Hong Kong Med J. 2006 Aug;12(4):264-71]. Perforation is rarely seen in our experience but a recent surgical case series from South Africa in HIV positive patients included 4 with perforation [see World J Surg. 2007 May;31(5):1087-96]. Intestinal TB is usually an intraluminal disease that presents with fever, diarrhea, and sometimes intestinal obstruction. Intestinal TB is distinct from peritoneal TB [see Gorgas Case 2004-04], which is thought to most often occur by seeding after rupture of and intra-abdominal lymph node. There are three ways for bacilli to reach the intestine (ingestion, hematogenous and spread from a contiguous focus); the hematogenous route is most likely in this case. There are three macroscopic forms of intestinal TB; ulcerative (most common), hypertrophic and mixed. Involvement of the ileocecal region is most common (90% of all intestinal cases), usually accompanied involvement in draining lymph nodes. This patient has disseminated TB (pulmonary, lymph node, intestinal) and the HIV and the lack of granulomas indicate a low CD4-count (not available yet). Treatment includes antibiotics as would be used for any interstinal perforation plus standard TB therapy. HAART is deferred until completion of the first 2 months of TB therapy in order to avoid a severe immune reconstitution syndrome in a patient with such a high bacillary load. HIV increases risk of progression of those infected with TB to active tuberculosis (10% per year in HIV positive vs. 10% life-time in HIV negative individuals). In Perú, approximately 40% of HIV patients develop active TB at some time. Conversely, TB infection induces increased HIV replication. HIV is the leading cause of hospitalization on our Infectious Diseases unit; TB is the leading opportunistic infection in these patients. The clinical presentation of TB varies according to CD4 count. Typical pulmonary disease with cavities is seen in patients with CD4>200, disseminated (more than one focus or hematogenous spread) with bilateral pulmonary infiltrates and mediastinal-pleural involvement is seen in those with lower CD4 counts and especially with < 100 CD4 cells. A positive PPD in HIV-infected patients with miliary TB is seen in less than 10%, positive sputum smears are seen only in 25%, blood cultures tend to be positive in 50-60%. Post-operatively this patient was treated with broad spectrum antibiotics and 4-drug TB therapy. The course was complicated by dehiscence of the anastomoses requiring an ileostomy. Fistula to adjacent organs, dehiscence of sutures, sepsis, malnutrition and high mortality are reported in these patients. |