| 2009 Case #1 |  |
|
|
The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Perú. For the ninth consecutive year, we are pleased to share interesting cases seen by the participants that week during the February/March course offerings. Presently the 9-week Gorgas Course in Clinical Tropical Medicine is in session. New cases will be e-mailed every Monday/Tuesday for the next nine weeks. Each case includes a brief history and digital images pertinent to the case. A link to the actual diagnosis and a brief discussion follow. David O. Freedman & Eduardo Gotuzzo |
| The following patient was seen in the outpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital. We thank Dr. Alejandro Llanos and his staff for advice and collaboration in this presentation. |
|
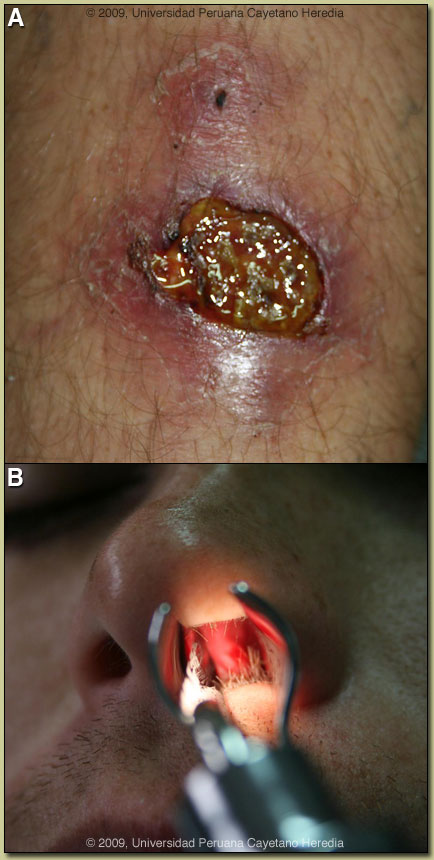
Epidemiology: Born in Lima and lived in Piura in Northern Perú until moving in October 2007 to Madre de Dios to a field station bordering Manu National Park. Physical Examination: Afebrile. Large ulcerated lesion with raised borders and a clean base on the left leg with small satellite lesions [Image A]. On examination with a nasal speculum a small ulcer with erythema and raised borders was noted on the middle third of the nasal septum [Image B]. Indirect laryngoscopy was negative. Chest was clear. No lymphadenopathy or hepatosplenomegally. Laboratory Examination: Normal chest x-ray. Normal hematology and liver function. Diagnostic procedures were performed on the lesions.
|
| Diagnosis: Mucocutaneous leishmaniasis due to Leishmania braziliensis. |
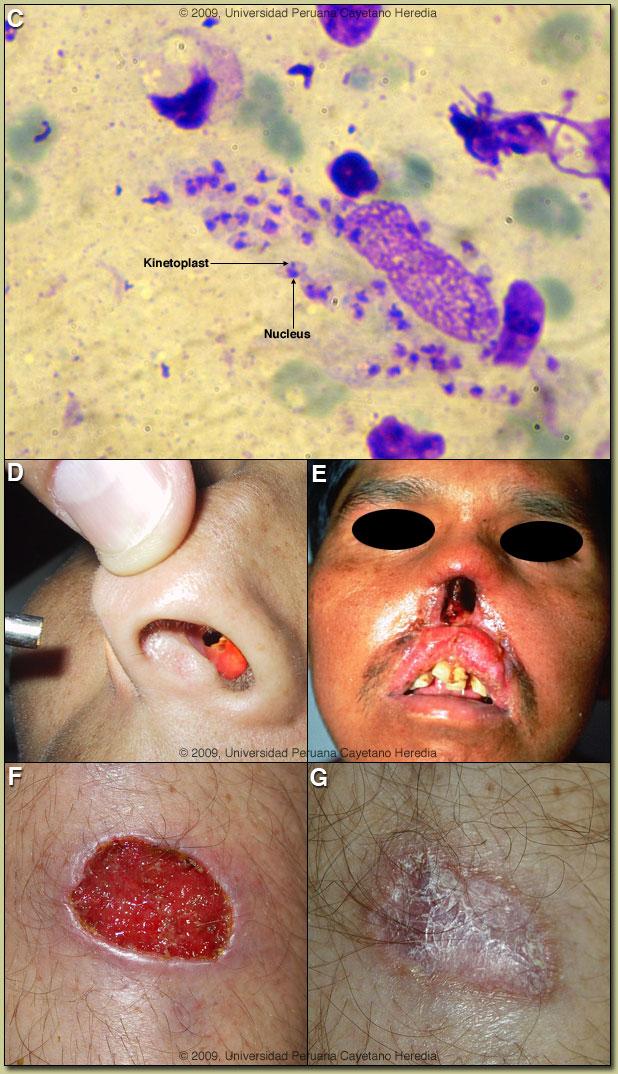 Discussion: The raised border of the ulcer was scraped with a scalpel blade and Image C shows a giemsa-stained smear of the scraping demonstrating a single macrophage with many typical intracellular amastigotes of Leishmania. Amastigotes are rounded organisms with the diagnostic and sometimes elusive finding of a kinetoplast (specialized DNA) that is very small and completely distinct from the nucleus. A culture of a needle aspirate of the raised border of the leg ulcer was positive for Leishmania and PCR of the culture confirmed infection with L. braziliensis. PCR of a sample taken from the nasal septum was also positive for L. braziliensis. Discussion: The raised border of the ulcer was scraped with a scalpel blade and Image C shows a giemsa-stained smear of the scraping demonstrating a single macrophage with many typical intracellular amastigotes of Leishmania. Amastigotes are rounded organisms with the diagnostic and sometimes elusive finding of a kinetoplast (specialized DNA) that is very small and completely distinct from the nucleus. A culture of a needle aspirate of the raised border of the leg ulcer was positive for Leishmania and PCR of the culture confirmed infection with L. braziliensis. PCR of a sample taken from the nasal septum was also positive for L. braziliensis.
L. braziliensis only occurs in the Americas and is the only Leishmania species that causes mucocutaneous disease. In this part of the world the vector is the Lutzomyia sandfly. The urban areas of Piura where the patient was living previously are not endemic for leishmania. While L. braziliensis is the only leishmania species present in this area of the jungle, in South America it is important to definitively distinguish Leishmania species that cause only cutaneous disease (L. peruviana in Perú) from the mucocutaneous species. Both typically cause one or a few initial skin lesions that are ulcerative but painless in nature and that usually spontaneously heal over time. However, with L. braziliensis (the mucocutaneous species), severe destructive recurrence may occur in the mucosal surfaces of the naso- and oropharynx from months to years after treatment or healing of the skin ulcers. The destructive lesions remain painless so many patients may not present until advanced disease and obstructive symptoms are present. This case is unusual because of the simultaneous appearance of skin and mucosal lesions, which occurs in less than 3% of even carefully studied patients [Am J Trop Med Hyg. 2006 Aug;75(2):267-9]. Mucosal lesions usually occur after a clinical cure of the initial cutaneous site of infection likely as a result of metastatic spread of the parasite. Then, mucosal involvement is not normally recognized by the patient until significant destruction of nasal or oropharyngeal tissue occurs. It is important to check patients presenting with mucosal disease for cutaneous scars indicative of earlier healed lesions. Our patient had no such scars and had never before been in an endemic area. For comparison, more advanced lesions from our files are shown in Images D and E. Nasal septal perforation is commonly the next step in the evolution and with advanced disease more severe destructive lesions occur. The major differential diagnosis in Perú of oro-pharyngeal lesions would be paracoccidioidomycosis, carcinoma, or lymphoma. In Perú leishmaniasis would be by far the most common. The painless nature of the mucosal lesions despite widespread destruction of tissue and involvement of the nasal mucosa, as well as spread to the larynx are consistent only with leishmaniasis. Distinguishing L. braziliensis from L. peruviana has usually involved laborious culture techniques followed by electrophoretic isoenzyme analysis. A new microculture technique has shown promise for ease of use and sensitivity in our hands though insufficient parasite material for further speciation is obtained [Am J Trop Med Hyg. 2008 Dec;79(6):847-52]. Investigators at our institute have published a PCR assay [Clin Infect Dis. 2006 Mar 15;42(6):801-9] for distinguishing the 2 species from the initial skin lesions. Early identification of the species that causes the initial cutaneous infection would greatly help to prevent mucocutaneous leishmaniasis, because it would allow more aggressive treatment and follow-up. In Perú L. peruviana (cutaneous disease only) occurs only in the high Andes; L braziliensis occurs only in the jungle and in the Amazon. As for all mucosal cases, the patient received 30 days of a pentavalent antimonial (meglumine-antimoniate 20mg/kg/d intravenously). Monitoring for failure of initial therapy is done clinically. Lesions that don’t respond at all by the end of the therapy course or don’t cure completely by 3 months should be considered failures and treated with another drug. In Perú, patients with initial presentation of mucosal disease do not always respond to antimony. Both clinical and parasite factors may contribute to antimony treatment failures [Clin Infect Dis. 2008 Jan 15;46(2):223-31]. In this case, the skin ulcer improved significantly with treatment; see Images F and G for the resolution at Days 30 and 60. There was some initial improvement of the mucosal lesion, but after 60 days it was larger than at pre-treatment and Amphotericin B (0.7 mg/kg/d, IV) was begun to continue to a total cumulative dose of 25 mg/kg. The patient developed hypokalemia despite pre- and post-treatment hydration and supplemental potassium but has tolerated 3 times per week dosing with the same target cumulative dose. A second course of antimony was an option but the patient had developed severe myalgias and nausea on that drug. Liposomal amphotericin may be used in resource rich settings but based on limited trials is not better in terms of efficacy even if less toxic.
|