| 2011 Case #6 |  |
|
| This patient was seen on the outpatient department of the Tropical Medicine Institute. We would like to thank Clinton White, University of Texas Medical Branch at Galveston, and Hector Hugo-García, Lima, Perú, for discussion and advice on the case. |
|
Epidemiology: Born and lives in Lima. Sporadic visits to rural farming areas in the highlands to visit family. No known TB exposures or HIV risk factors. Physical Examination: Afebrile. BP 110/60, HR 70, RR 16. Multiple firm mobile subcutaneous nodules of 1-2 cm on the scalp, trunk, extremities, and face, with normal overlying skin [Images A (leg) and B]. Chest clear. CVS normal. No organomegaly or lymphadenopathy. CNS: no fundus abnormalities or papilledema, normal cranial nerves, normal motor and sensation. Laboratory Results: Hematocrit 35%. WBC 7.5 (50 PMN, 30 lymphs, 8 monos, 10 eosinophils, 2 basophils). Liver function normal. A biopsy of a skin lesion was performed [Image C].
|
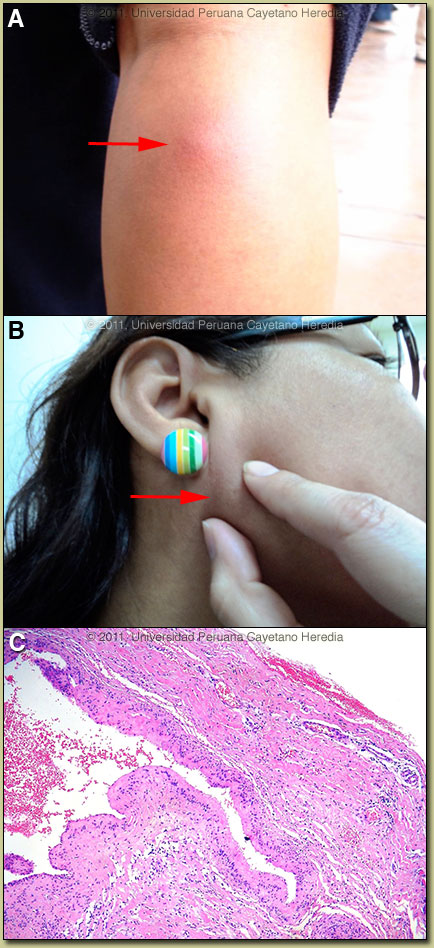 History: 45 year old woman with a 2 year history of progressive development of slightly tender papules and nodules that continue to appear throughout the body including face, neck, trunk, scalp, and extremities. On no medications. No ulceration or discharge from any lesions. Sporadic headaches – some lasting for days – have occurred in the past 4 years. No fever, weight loss or systemic symptoms. No past illnesses.
History: 45 year old woman with a 2 year history of progressive development of slightly tender papules and nodules that continue to appear throughout the body including face, neck, trunk, scalp, and extremities. On no medications. No ulceration or discharge from any lesions. Sporadic headaches – some lasting for days – have occurred in the past 4 years. No fever, weight loss or systemic symptoms. No past illnesses.| Diagnosis: Neurocysticercosis due to Taenia solium. Cysticerci in soft tissue. |
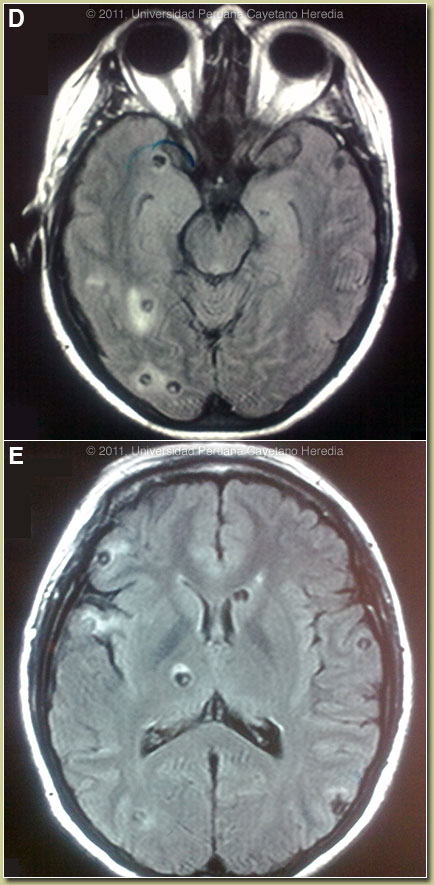 Discussion: The biopsy showed a large cystic structure with a homogenous histiocytic wall and eosinophils surrounding the cystic space. Western blot was positive for cysticercosis. MRI of the brain showed at least 30 cysts with perilesional edema and a hyperintense intracystic point on FLAIR images corresponding to the scolex of the larvae [Images D and E]. No intraventricular lesions or signs of intracranial hypertension were seen. No calcified lesions were seen on CT scan (not shown). Discussion: The biopsy showed a large cystic structure with a homogenous histiocytic wall and eosinophils surrounding the cystic space. Western blot was positive for cysticercosis. MRI of the brain showed at least 30 cysts with perilesional edema and a hyperintense intracystic point on FLAIR images corresponding to the scolex of the larvae [Images D and E]. No intraventricular lesions or signs of intracranial hypertension were seen. No calcified lesions were seen on CT scan (not shown).
Cysticercosis is infection with the larval stages of the human pork tapeworm Taenia solium. Humans acquire cysticercosis after ingesting eggs of T. solium in material contaminated with feces originating in human tapeworm carriers. Humans that do not eat pork can get cysticercosis. Ingestion of contaminated pork results in humans getting an adult intestinal tapeworm – not cysticercosis. Cysticercosis is common in many developing countries and very common in rural agricultural areas of Perú. In developed countries, the long-lived cysticerci are increasingly seen as immigration from affected areas rises. Occasional transmission by tapeworm carriers to those who have never left non-endemic countries is reported. Ingested T. solium eggs hatch in the stomach and are then carried to the muscles and other tissues where the larvae encyst and reach their usual size of about 1 cm within a few months. Clinical manifestations depend on the affected organ, but neurocysticercosis causes the most morbidity. The cysticerci seem able to evade the immune system and are thought to remain viable for several years without causing any inflammatory response. Most clinical symptoms are the direct result of inflammatory responses that accompany the eventual cyst degeneration. Epileptic seizures are the primary or sole clinical manifestation in up to 80% of patients. In endemic regions, new onset seizures in teenagers or young adults are most likely due to neurocysticercosis. Cysticerci can also cause symptoms because of mass effect, impingement on a vital structure, or blockage of CSF circulation, especially if the cyst is intraventricular. In this patient with widespread seeding of the body, we cannot rule out the presence of cysts in or near important structures. This has potential implications for inflammatory reactions induced by anti-parasitic treatment. In the brain, one potentially problematic cyst is noted in the Right thalamic area. Treatment of parenchymal neurocysticercosis with antiparasitic drugs such as albendazole is increasingly accepted, even when there are few lesions. Albendazole kills cysts, but may lead to added inflammation and exacerbation of symptoms, which is usually dealt with by empiric concomitant use of steroids. Considerations in patients such as this, with large numbers of active lesions, include severe inflammation due to simultaneous killing of many organisms, include more aggressive, higher dose or extended steroid therapy. Therapeutic decisions should be based on the number, location, and viability of the cysts. Patients in whom all lesions are already calcified should receive no anti-parasitic treatment. Recent work indicates that long-standing calcified lesions can sometimes provoke peri-lesional edema, which may need treatment with steroids as well as anti-seizure medication. Neurocysticercosis is a variable disease and treatment approaches need to be individualized to a large number of differing clinical presentations [Neurology. 2006 Oct 10;67(7):1120-7]. In all cysticercosis patients, seizures need to be managed as per any other form of epilepsy. For our patient we have recommended treatment with prolonged albendazole for 30 days under steroid cover. Current practice of shorter courses of 8-10 days has been called into question due to the limited (30-50%) resolution of cystic lesions at 6 months with no impact on calcifications with these regimens [N Engl J Med. 2004 Jan 15; 350(3):249-58]. This is likely an even more important consideration in those with high cyst burden, though there is no specific data on 30 days of therapy. We use dexamethasone 12mg/day for 10 days then 8 mg/day during the remainder of the albendazole course; this may need modification according to patient response.
|