| 2011 Case #11 |  |
|
|
This is our last case of the week for 2011. We hope you have enjoyed the 2011 series of live cases each week from Perú. The Gorgas Diploma Course is held annually in February and March and we will be in touch at the beginning of next year’s case series. Eduardo Gotuzzo, M.D. and David O. Freedman, M.D. |
| The following patient was seen by Gorgas Course participants on the 36-bed inpatient ward of the Tropical Medicine Institute. |
|
Epidemiology: Born and lives in Tumbes on the north coast of Perú. He works selling agricultural goods with daily border crossings into Ecuador. No other history of travel; never visited the jungle. Frequent swimming in a local river. No known TB exposure; no specific HIV risks. Physical Examination: Afebrile, normal vital signs. Chest clear. No hepatosplenomegaly or lymphadenopathy. 9 x 5 cm ulcer over right knee [Image A]. Borders are undermined allowing a cotton swab to be inserted [Image B]. Mild pain on pressing intact border over the tibia. No mucosal lesions. Laboratory Results: Hemoglobin 13.7; WBC 8730 (normal differential); normal biochemistry. X-ray of the knee: normal; no bone or articular involvement. |
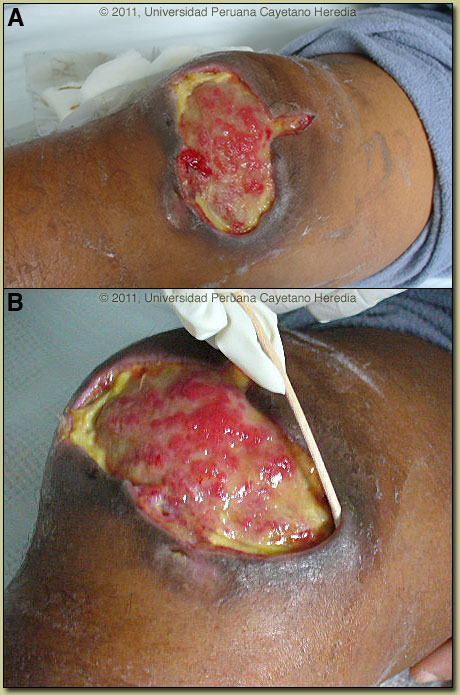
| Diagnosis: Buruli ulcer caused by Mycobacterium ulcerans. |
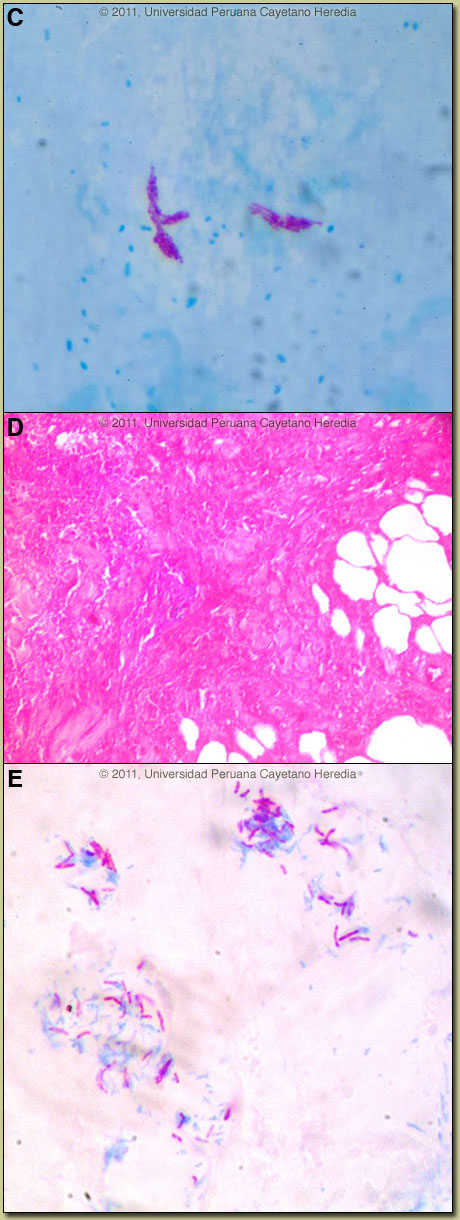 Discussion: Acid fast staining of a touch prep taken from the bottom of the ulcer directly onto a glass slide is shown [Image C] and demonstrates AFB extracellularly and in clusters. Histopathology of a biopsy specimen shows characteristic extensive necrosis of the subcutaneous tissue with extension to the dermis [Image D]. The Ziehl-Neelsen and the Fite Faraco stains of the biopsy were both positive for AFB [Image E]. Culture and PCR are pending. All other cultures and special stains for fungi, bacteria, and leishmania were negative. According to WHO consensus criteria for laboratory diagnosis of Buruli ulcer, any 2 of the following 4 criteria are sufficient: (1) acid-fast bacilli in a stained smear; (2) positive mycobacterial culture (requires 6-8 weeks); (3) positive PCR; (4) typical histopathology in an excisional biopsy. Estimated sensitivities for these techniques range from 60% or less to more than 90%, but WHO considers the possibility that one positive result might be sufficient in a context of a high clinical suspicion. Discussion: Acid fast staining of a touch prep taken from the bottom of the ulcer directly onto a glass slide is shown [Image C] and demonstrates AFB extracellularly and in clusters. Histopathology of a biopsy specimen shows characteristic extensive necrosis of the subcutaneous tissue with extension to the dermis [Image D]. The Ziehl-Neelsen and the Fite Faraco stains of the biopsy were both positive for AFB [Image E]. Culture and PCR are pending. All other cultures and special stains for fungi, bacteria, and leishmania were negative. According to WHO consensus criteria for laboratory diagnosis of Buruli ulcer, any 2 of the following 4 criteria are sufficient: (1) acid-fast bacilli in a stained smear; (2) positive mycobacterial culture (requires 6-8 weeks); (3) positive PCR; (4) typical histopathology in an excisional biopsy. Estimated sensitivities for these techniques range from 60% or less to more than 90%, but WHO considers the possibility that one positive result might be sufficient in a context of a high clinical suspicion.
Mycobacterium ulcerans is the third most common mycobacterial infection worldwide (after tuberculosis and leprosy). WHO has recognized Buruli ulcer as a public health problem in West and Central Africa, with highest incidence rates in Benin, Ghana, and Ivory Coast. However, Buruli ulcer is reported in over 30 countries including Australia [see Dermatol Clin. 2009 Jan;27(1):63-73. Review.]. Buruli ulcer is commonest in rural tropical wetlands, especially areas with stagnant water, including ponds and swamps. Our group has now seen 15 cases infected in Perú including 8 previously published [see Emerg Infect Dis. 2008 Mar;14(3):373-7. and Gorgas Case 2003-09]; most cases come from Amazonian jungle areas and the rest come from the northern coastal areas. Clinically the disease is divided into ulcerative and non-ulcerative forms, and the non-ulcerative forms don’t necessarily progress to ulcerative disease. Non-ulcerative forms present as papules, nodules, plaques, or in a diffuse edematous form with non-pitting swelling. The ulcerative form when fully developed has broadly undermined edges and is indurated peripherally. The ulcer is usually painless unless there is bacterial superinfection. When more than one ulcer is seen they are close together and usually communicate under the intact skin. Contractures may occur as a complication of scarring of lesions occurring over or close to joints. Osteomyelitis may occur in up to 10% due to primary spread or as a metastatic process. Systemic signs are rare. Although the clinical diagnosis of the ulcerative form is straightforward, it is more difficult for the nodule, plaque, and oedematous forms. Tropical phagedenic ulcer (due to fusobacteria and spirochetes) and necrotizing fasciitis are painful and aggressive. Neither leishmania nor sporotrichosis would be undermined around the edges and generally would manifest some lymphatic spread by this stage. M. tuberculosis and other mycobacteria cause granulomatous and not necrotizing disease. The pathogenesis of the disease is thought to relate to inoculation of the organism from the environment into subcutaneous tissues after trauma to contaminated skin sites. Human to human transmission is thought not to occur. Pathogenesis is mediated by mycolactone, a diffusible, necrotizing, immunosuppressive, polyketide-derived macrolide toxin secreted by M. ulcerans. Mycolactone has an affinity for fat cells and causes progressive radial necrosis of subcutaneous tissues (clinically manifest by the undermined ulcer border) and subsequently, but more slowly, the overlying skin breaks down. In tissues, M. ulcerans grows primarily as extracellular microcolonies and not as facultative intracellular parasites as do other mycobacteria. Excisional biopsies (punch biopsy should not be used) that sample the full thickness of the skin down to the fascia are required and should be taken from the edge of the skin surrounding an ulcer or from the middle of a papular or nodular lesion. M. ulcerans shares some environmental, molecular, and clinical features with Mycobacterium marinum, another water-associated organism but which causes granulomatous skin lesions in humans. Genetic analysis indicates that M. ulcerans likely diverged from M. marinum, acquiring a virulence plasmid with genes coding for mycolactone production. Some taxonomists consider all mycolactone-producing mycobacteria as M. ulcerans even if an individual isolate shares some features with other mycobacteria [see PLoS Negl Trop Dis. 2010 Jul 27;4(7):e663]. Historically, treatment of Buruli ulcer was limited to wide surgical excision of the affected tissues. In 2004, WHO advocated a provisional antibiotic regimen comprising oral rifampin (10 mg/kg) plus intramuscular streptomycin (15 mg/kg), both given daily for 4-8 weeks under supervision depending on disease stage [for details see Lancet Infect Dis. 2006 May;6(5):288-96. Review.]. Amikacin (15 mg/kg) can be substituted for streptomycin, administered intramuscularly or intravenously. Surgery is still necessary for more advanced disease in combination with drug therapy. According to WHO guidelines, those with lesions 5 to 15 cm in diameter (category II, moderate), such as our patient, receive 4 weeks of antibiotics and then undergo surgery, if necessary, followed by 4 more weeks of antibiotics. Fully oral, less-toxic regimens, such as rifampin plus clarithromycin or rifapentine plus moxifloxacin are under investigation. Of note is that several of our cases in Perú have followed indolent courses or have healed with no treatment; at the same time isolation of the causative agent in our cases has been elusive. Genetic differences between strains from different parts of the world, which are being described, could explain these findings but remain to be further investigated. |