| 2012 Case #1 |  |
|
|
The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Perú. For the 12th consecutive year, we are pleased to share interesting cases seen by the participants that week during the February/March course offerings. Presently the 9-week Gorgas Course in Clinical Tropical Medicine is in session. New cases will be posted every Monday/Tuesday for the next nine weeks. Each case includes a brief history and pertinent digital images, followed by a link to the actual diagnosis and a brief discussion. David O. Freedman & Eduardo Gotuzzo |
| The following patient was seen in the Intensive Care Unit of the 450-bed Cayetano Heredia National Hospital. |
|
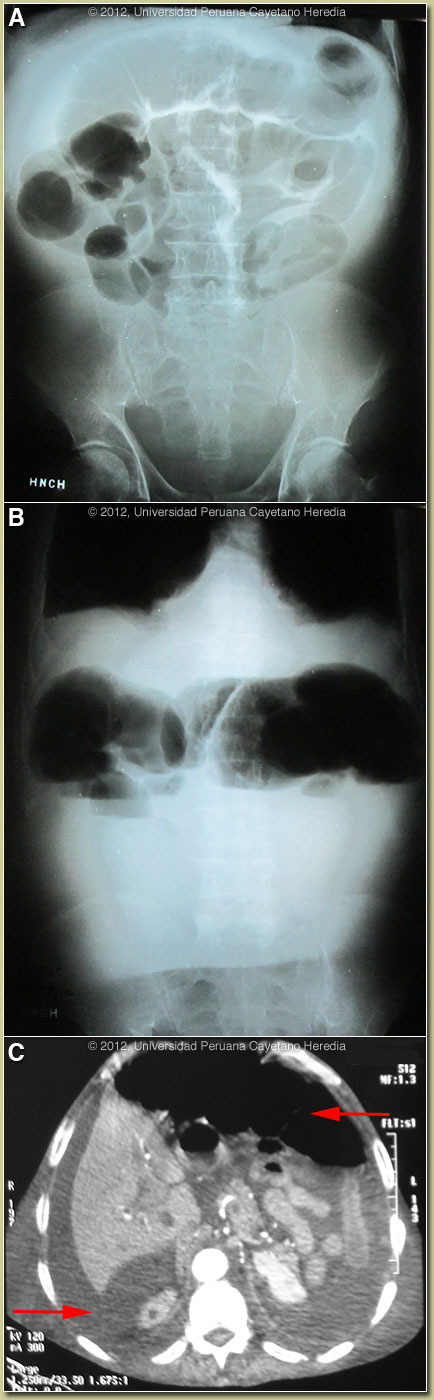
Epidemiology: Farmer, born and lives in Ayacucho in the Andean highlands. Has cows, pigs, chickens and horses. No running water or drainage. Light smoker; occasional alcohol use. No known exposure to TB or blood pathogens. Physical Examination (on admission): BP 90/60, HR 70, RR 15, T 36.5 °C, O2Sat 95%. Somnolent, pale, and dehydrated. Chest: bilateral crackles. Abdomen: slightly active bowel sounds; soft, non-distended, shifting dullness. No hepatosplenomegaly. Extremities: bilateral lower limb edema. Laboratory Results: Hb 11.2, Hct 34, WBC 2900, PMN 54, bands12, Eos 0, Monos 10%, Lymphs 24, platelets 175,000, Glucose 104, BUN 128, Creatinine 1.7, Total protein 4.0, albumin 1.5 (N>3.5), Bilirubin 0.5 (direct 0.4), ALT 23, AST 32, GGT 10, LDH 794. HbsAg and Anti-HCV negative. Sputum for AFB negative. Chest x-ray: small left pleural effusion, normal lung parenchyma. Evolution: The patient was treated initially for sepsis but over the next days, developed severe painful abdominal distension with hypotension requiring pressors. Abdominal x-ray [Images A and B] disclosed edema of the small and large bowel with air-fluid levels in the colon. Abdominal CT scan with oral contrast [Image C] showed dilated air filled sigmoid colon anteriorly (arrow), and dilated small bowel loops and severe ascites posteriorly (arrow). He remained afebrile. He was taken to laparotomy with a diagnosis of large bowel obstruction. |
| Diagnosis: Balantidium coli. Secondary bacterial sepsis. |
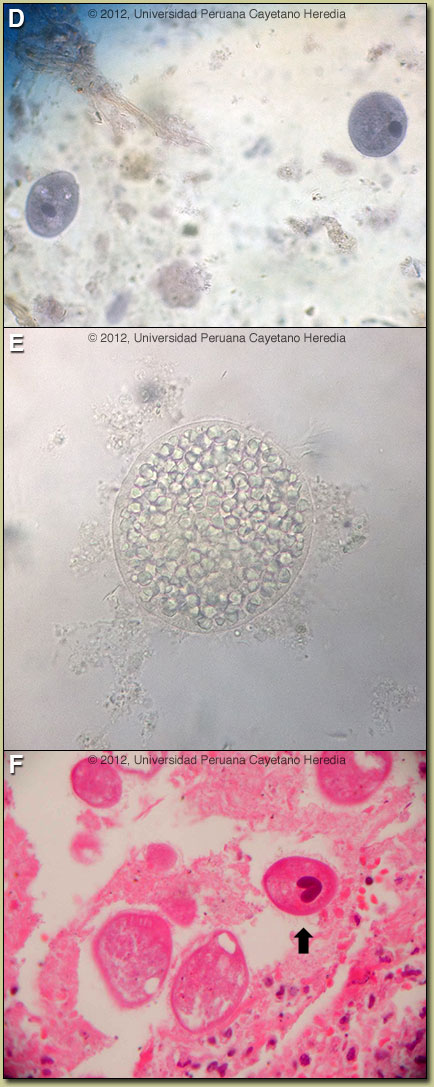 Discussion: At laparotomy, ileus with dilated edematous bowel with no obstruction or perforation was found and no surgical procedure was performed. Examination of a stool specimen showed both trophozoites [Image D] and cysts [Image E]; no macronucleus visible in this specimen) of Balantidium coli. Image F shows a tissue section from a previous case of the week [see Gorgas Case 2002-07] that presented with colonic perforation; an organism with the characteristic kidney or sausage-shaped macronucleus (arrow) is visible and the pathognomonic cilia can also be distinguished. Trophozoites are typically more pointed at the anterior end. Rounded cyst forms only are found in stool specimens in asymptomatic cases, but in patients with clinical manifestations generally trophozoites predominate. Acid fast stain of stool was negative for Cyclospora, Cryptosporidium, or Cystoisospora. HIV was negative. Discussion: At laparotomy, ileus with dilated edematous bowel with no obstruction or perforation was found and no surgical procedure was performed. Examination of a stool specimen showed both trophozoites [Image D] and cysts [Image E]; no macronucleus visible in this specimen) of Balantidium coli. Image F shows a tissue section from a previous case of the week [see Gorgas Case 2002-07] that presented with colonic perforation; an organism with the characteristic kidney or sausage-shaped macronucleus (arrow) is visible and the pathognomonic cilia can also be distinguished. Trophozoites are typically more pointed at the anterior end. Rounded cyst forms only are found in stool specimens in asymptomatic cases, but in patients with clinical manifestations generally trophozoites predominate. Acid fast stain of stool was negative for Cyclospora, Cryptosporidium, or Cystoisospora. HIV was negative.
Balantidium coli is the largest protozoan and the only ciliate parasite that infects humans. Many animal species harbor the organism as an intestinal commensal but pigs have a particularly high rate of infection and are usually considered to be the main reservoir of this organism. B. coli’s habitat in humans is the cecum and colon. B. coli appears to have a worldwide distribution but is considered an uncommon human infection. However, most of the literature (1,000 cases or so) is concerned with individual symptomatic or complicated cases. A small number of population-based studies including from Bolivia and Ecuador have reported prevalances of 1-6% in asymptomatic individuals in highly endemic areas such as the Andean altiplano [see Am J Trop Med Hyg. 1998;59:922-7.], Papua New Guinea, and the Philippines. Thus, it appears that humans are quite refractory to infection with this ubiquitous porcine parasite and the factors that result in severe disease in a very small number of individuals are not clear. Our patient had no apparent underlying disease or risk factors. Interestingly, numerous attempts have been made over the years to experimentally infect humans with significant numbers of B. coli organisms isolated from various animals, but they have been unsuccessful. Transmission is thought to be via contamination of water supplies by pig feces or by direct contact with pigs. Human-to-human transmission has been reported. In the sporadic cases that have clinical manifestations, stools may be either watery or dysenteric. Fulminant disease presents rarely and is most associated with fulminating dysentery with or without multiple intestinal perforations. When present, the colonic ulcers and clinical presenation are similar to those found in amebic dysentery/peritonitis with deep invasion of submucosa with organisms. Microperforations with resulting sepsis are thought to occur and to account for presentations similar to this case. Occasional involvement of appendix and terminal ileum have been reported but this is a predominantly colonic process. The other major diagnostic consideration in a case of infectious peritonitis or intestinal perforation in this setting would be amebic disease. Pyogenic abscess due to a ruptured diverticulum or appendix or tuberculous peritonitis would have been accompanied by fever from the outset. Tetracycline is generally considered to be the drug of choice, but successful therapy with metronidazole or iodoquinol has been described. The patient continues afebrile but requiring pressors and ventilation. He is currently receiving metronidazole and meropenem. A recent review on B. coli can be found at Clin Microbiol Rev. 2008;21:626-38. |