 |
Gorgas Case 2021-04 |
|
The following patient was seen as an outpatient at a private clinic in Lima. 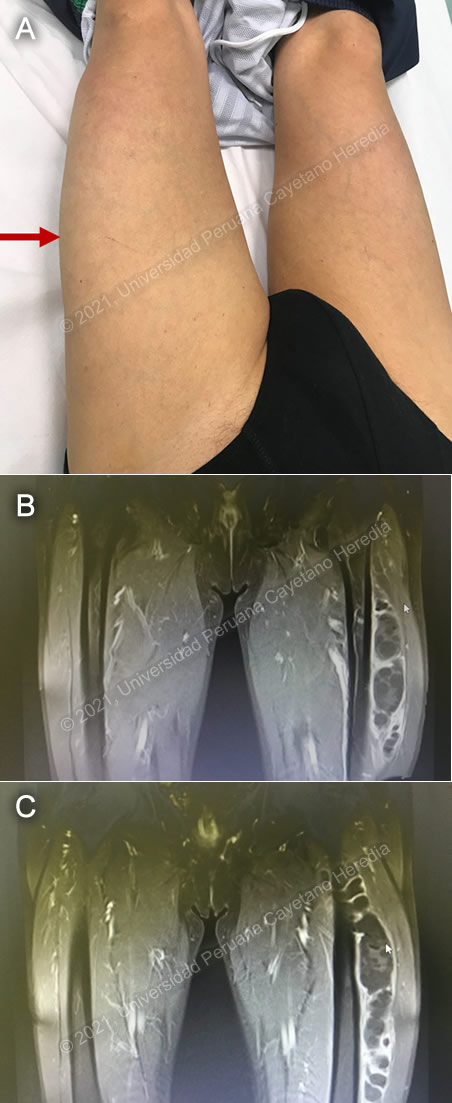 History: A 75-year-old male patient was transferred from a hospital in the highlands of the country to a private clinic in Lima for further evaluation of progressive swelling of the left thigh that ensued over the last 5 months. The lesion was painless, it was not associated with systemic symptoms or physical impairment, and was not related to previous trauma, he also denied similar lesions in other parts of the body or a previous febrile episode. He remembered to have had a similar but smaller lesion in the left thigh in 2016 that was treated with unknown antibiotics with full resolution. Epidemiology: Born and lives in Huancayo, a city in the highlands of Peru. He works as a farmer and was in contact with dogs, cats, guinea pigs and pigs throughout his life. Denies any recent travel. Denies contact with TB patients. Physical Examination: Afebrile with normal vital signs, the patient appears in no distress. There was a non-tender soft swelling of the left thigh with no inflammatory signs on the overlying skin. (Image A). Chest and cardiovascular examinations were normal. No organomegaly. Normal neurologic examination. Imaging studies: Chest x-ray was normal. MRI of the left leg is shown in Images B and C. The abdominal ultrasound was reported as normal. Laboratory Examination: Hb: 13.7 g/dL; Hct. 40%; WBC 7 650 (neutrophils: 60%, eosinophils: 0, lymphocytes: 35%); Platelets: 236 000. Gluc: 108 mg/dL, Creat: 0.9 mg/dL, AST 33 U/L, ALT 27 U/L, albumin 3.9 g/dL.
|
|
Diagnosis: Primary skeletal muscle hydatidosis caused by Echinococcus granulosus 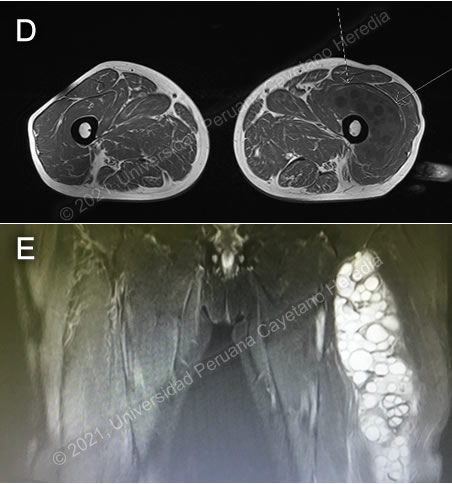
 Discussion: The serum Western-Blot for E. granulosus infection was positive. The MRI of the left leg shows (T1 sequence with contrast) the presence of a large hydatid cyst with daughter cysts inside located in the left thigh (Images B and C). Additional images at the T1 sequence without contrast reveals that a large cyst is located in the intermediate vast of the quadriceps femoris muscle, the T2 weighted sequence revealed high signal intensity characteristic of the liquid component of the cysts (Images D,E). On further questioning, he remembered that at the age of 14 years a small cyst was identified in his right upper lung, medical treatment was offered but he does not remember further clinical or therapeutic details. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. This patient had ongoing exposure to dogs during his entire life. Sheep are the normal intermediate hosts. In general, disease is diagnosed in adulthood as larval cysts expand slowly over years or decades, becoming symptomatic as they impinge on other structures by virtue of their size. The cysts contain hundreds of viable protoscoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new protoscoleces on an ongoing basis and may also produce internal daughter cysts. Each protoscolex is capable of becoming a new cyst should the original cyst rupture or be ruptured. Cystic hydatid disease due to E. granulosus is common in sheep and cattle raising areas worldwide. Most primary infections involve a single cyst. In adults, 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen (see case #7, 2009), heart, bone, muscles and brain (see case #5-2014). This is the first case of a well-documented skeletal muscle hydatidosis presented as a case of the week since we started posting cases in 2001. |