 |
Gorgas Case 2026-2 |
|
The following patient was seen on the inpatient ward of Cayetano Heredia Hospital in Lima by the 2026 Gorgas Course participants.
 History: A 60-year-old male from Lima presented with a 6-year history of a progressively enlarging left nasal lesion and dysphagia. The lesion initially appeared as a painless papule with mild pruritus that gradually increased in size. By the fifth year of disease, the lesion became pustular after self-manipulation, with progressive growth and blood-tinged discharge. The nasal lesion became crusted and extended bilaterally, causing partial nasal obstruction, sleep-related breathing difficulty, nasal discharge, hoarseness, and dysphagia. In the last seven months, he noticed worsening of the symptoms. Due to the burden and progression of symptoms, he sought medical attention and was subsequently hospitalized. Epidemiology: The patient was born in Lima and currently resides in the district of Carabayllo, where he works as a construction worker. Travel history includes Aguaytia, a city in the high jungle of Peru, where he went thirty-two years ago and stayed for two years, working as a farmer harvesting bananas and cassava. In his second year, he developed a painless, ulcerative lesion with regular, elevated borders on the elbow. He didn’t seek medical care, and it self-limited in approximately three months, leaving an atrophic, hypochromic scar with irregular edges. He reports that during his stay, many of his co-workers presented similar lesions. Past medical history is notable for pulmonary tuberculosis, diagnosed seven months prior to admission after he developed cough, dyspnea, and weight loss. He completed treatment. Physical examination: HR: 81 x’, RR: 17 x’, BP: 102/66, Temp: 36.5, SatO2: 97%, FiO2: 0.21. The patient presents with marked nasal abnormalities, including an infiltrative, ulcerated lesion with irregular borders measuring approximately 3 × 3 cm in the left nasal cavity, associated with deformity, partial amputation of the left nostril, and a nasal septum perforation. Oral examination reveals a granulomatous lesion involving the hard palate and a nodular lesion at the apex of the tongue (Images A and B). Cutaneous findings include an atrophic, hypopigmented scar with irregular borders measuring approximately 6 × 2 cm on the elbow (Image C). A mobile left cervical lymph node measuring approximately 1 × 1 cm was also noted. The rest of the exam was unremarkable. Laboratory: Initial laboratory findings included hemoglobin of 9.9 g/dL, a white blood cell count of 5.8 ×10⁹/L with 68.8% neutrophils, and a platelet count of 576 ×10⁹/L. The metabolic panel was normal (urea 35 mg/dL, creatinine 0.5 mg/dL, sodium 137 mEq/L, potassium 4 mEq/L, chloride 95 mEq/L, and glucose of 88 mg/dL). Liver function tests and coagulation tests were also normal. Serologic testing for HIV was negative. A Montenegro skin test was positive (15x15mm). Imaging: A chest X-ray showed a nodular bilateral pattern, predominantly. Marked laryngeal thickening and narrowing. A neck lateral X ray showed thickening of the oropharyngeal region with visible obstruction (Image D). A CT scan showed similar findings along with cervical lymph nodes (Image E). UPCH Case Editors: Carlos Seas, Course Director / Paola Nakazaki, Associate Coordinator |
|
 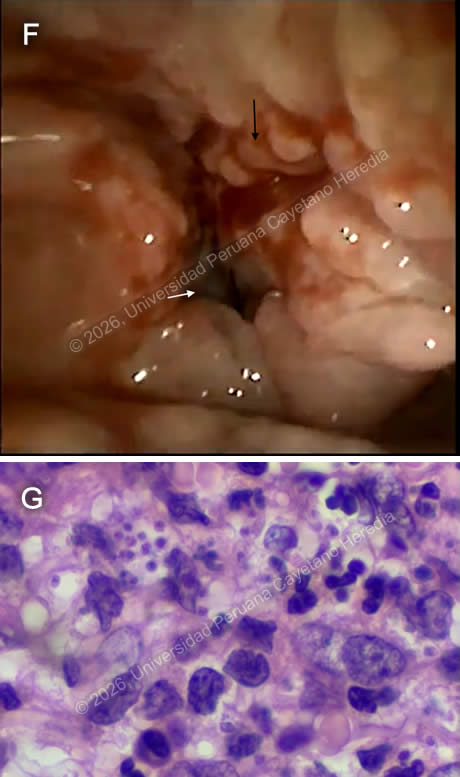 Discussion: The patient was diagnosed with extensive mucosal leishmaniasis. Significant clinical findings were noted after fiberoptic bronchoscopy, revealing a congested pharynx, epiglottis, and larynx with multiple friable granulomatous lesions, edematous vocal cords, and approximately 10% patency of the surrounding mucosal opening (Image F). A nasal mucosal biopsy demonstrated inflammatory infiltrates with fibrosis and intracellular structures morphologically consistent with amastigotes (Image G), confirming the diagnosis of mucosal leishmaniasis. Leishmaniasis is a vector-borne parasitic disease caused by Leishmania species, transmitted by infected female sandflies (Phlebotomus and Lutzomyia). It is endemic in tropical and subtropical regions. The World Health Organization reports an estimated annual incidence of 700,000 to 1 million new leishmaniasis cases, with the majority occurring in the African region and the Americas (1). It is an endemic infectious disease in Peru, Leishmania (Viannia) braziliensis is the principal etiologic agent of mucocutaneous leishmaniasis, with L. (V.) guyanensis, L. (V.) peruviana, and rarely L. (L.) amazonensis also reported (2). With more than 4,000 cases reported annually, it is predominant in rural areas of the jungle and highlands. The highest incidence is observed in the departments of Madre de Dios, Cuzco, Loreto, Ucayali, and Huanuco (3). This disease manifests in three main clinical forms: cutaneous, mucocutaneous, and visceral, with the cutaneous form being the most frequent. The clinical expression and severity of the disease are influenced by parasite, host, and vector-related factors (4). Mucocutaneous leishmaniasis most commonly presents as a late sequela of the cutaneous form, although concurrent presentation may occur (1). Approximately 90% of cases are associated with a history of prior cutaneous lesions, often evidenced by residual scarring, as in our patient’s case (Image C). Mucocutaneous leishmaniasis most commonly presents with nasal involvement, and as the disease progresses, lesions may extend to the oral cavity, palate, pharynx, or larynx; presenting with erythema, edema, infiltration, nodular or ulcerative lesions, and, in advanced cases, destructive changes (2). Diagnosis is based on clinical manifestations and epidemiologic factors, and is confirmed by identification of the species through microscopic examination of lesion aspirates or biopsies, culture, and molecular methods (5). Differential diagnosis includes paracoccidioidomycosis, tuberculosis, histoplasmosis, syphilis, rhinoescleroma, granulomatosis with polyangiitis, or extranodal T-cell lymphoma. Hospitalization was required for systemic treatment and observation due to our patient’s severe clinical presentation. Amphotericin B deoxycholate 0.7-1 mg/kg IV is recommended for extensive mucosal compromise and laryngeal and pharyngeal involvement (5, 6, 7). Despite the lack of large, randomized trials to guide dosing or duration, adjunctive short-term steroids may be recommended for patients with severe inflammatory disease and airway-threatening edema, with tapering guided by clinical response (2). ENT evaluation is also advised to manage and follow airway involvement (5). Our patient is receiving systemic treatment with Amphotericin B deoxycholate with a target of a cumulative dose of 25 mg/kg, and a course of steroids with significant clinical improvement. References |