 |
Gorgas Case 2026-3 |
|
The following patient was seen on the inpatient ward of Cayetano Heredia Hospital in Lima by participants in the 2026 Gorgas Course.
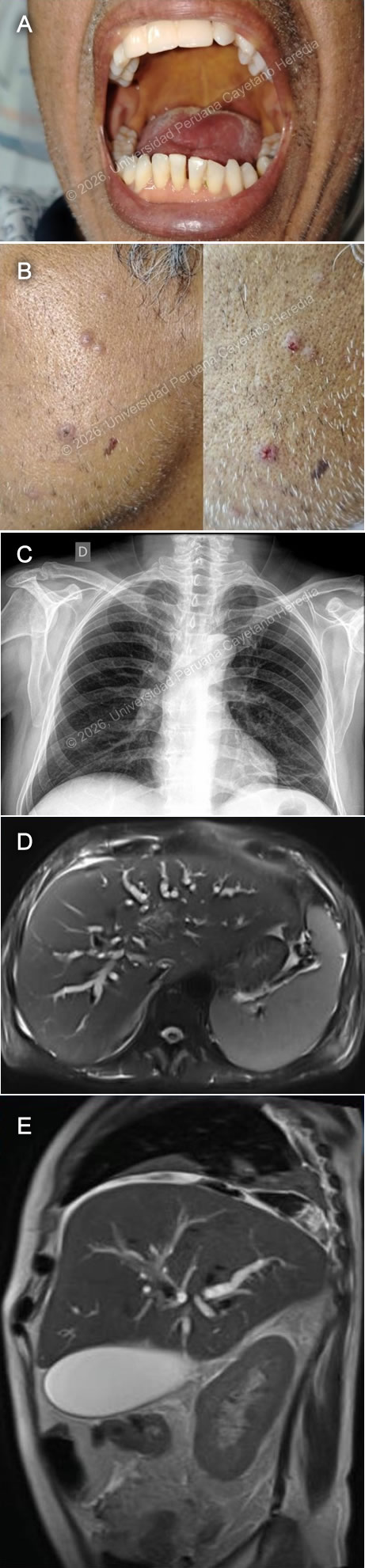 History: A 54-year-old man presented with a 3-month history of abdominal pain, weight loss, fever, and jaundice. Symptoms began with nausea and scleral/mucosal jaundice, and one month later, fatigue, poor appetite, postprandial epigastric pain, and bloating. He later developed pale stools, dark urine, night sweats, and fevers up to 38 °C. During the third month, he was empirically treated at a GI clinic with steroids (prednisone 40 mg/qd for one week) for a presumptive diagnosis of IgG4 disease. A week and a half later, he developed generalized lymphadenopathy and a papular skin rash. Worsening symptoms prompted an ED presentation and hospital admission for further evaluation. Epidemiology: The patient has a history of cutaneous leishmaniasis diagnosed and treated in 2022, which recurred in 2023 and healed with residual scarring. He was born in Yurumarca, Chachapoyas, in the high jungle of Peru. In adolescence, he moved to Lima. From 2020 to 2024, he lived and worked on a farm in Vituya, in the high jungle, where he cultivated dragon fruit, lemons, bananas, and oranges, and harvested coffee. He frequently swam in nearby rivers, visited caves while resting from farm work, raised multiple domestic animals, including guinea pigs, cattle, chickens, pigs, and donkeys, and reported exposure to rodents and bats. He consumed home-produced foods, including unpasteurized dairy products, and experienced frequent insect and mosquito bites. He denied known sick contacts, though neighbors reportedly had untreated skin lesions compatible with leishmaniasis. His home lacked electricity and potable water. Physical examination: HR: 103x’, RR: 21x’, BP: 120/80, Temp: 38°C, SatO2: 95% on room air. Clinical examination revealed jaundice of the skin, sclerae, and mucous membranes, along with pallor (Image A). Papular and crusted skin lesions were present on the face, submental region, and upper and lower extremities (Image B). An atrophic, hypopigmented scar was noted on the posterior left upper extremity. Oral examination revealed a full dentition without thrush or ulcers. Bilateral lymphadenopathy was noted, predominantly tender and soft, affecting the retroauricular, submandibular/submaxillary, axillary, and inguinal regions, with most nodes mobile and dry. The abdomen was distended, with right upper quadrant tenderness on palpation. The liver was palpable 3 cm below the right costal margin, and splenomegaly was noted. The rest of the exam was unremarkable. Laboratory: Basic analysis showed mild normocytic normochromic anemia with hemoglobin in 10.5 g/dL, with 8700 leukocytes (86% neutrophils, 8.6% lymphocytes, 1% eosinophils, 0.1% basophils, 4.3% monocytes). Glucose was 79 mg/dL. Renal function remained preserved (creatinine 0.7 mg/dL, urea 29–25 mg/dL), with normal electrolytes. Liver function tests were increased, with alkaline phosphatase of 920 U/L (Normal range: 40 to 129 U/L) and gamma-glutamyl transferase 1142 U/L (Normal range: 5-40 U/L), associated with total bilirubin of 17.4 mg/dL (Normal range: 0.1 to 1.2 mg/dL), with direct predominance (15 mg/dL). Liver transaminases were elevated AST/ALT: 119/120. Coagulation studies showed prolonged PT 25.6 and INR 2.07 and PTT 62. Lipid profile revealed hypercholesterolemia 219 mg/dL and hypertriglyceridemia 224 mg/dL. Amylase was 50 U/L (normal range: 30–140 U/L), lipase was 23 U/L (normal range: 0 to 160 U/L). Imaging: A chest X ray revealed mild bilateral accentuation of the bronchovascular markings, with no other significant findings (Image C), a magnetic resonance cholangiography showed marked dilation of the intrahepatic bile ducts secondary to diffuse mural thickening of the extrahepatic bile ducts, along with signs of hepatosplenomegaly, retroperitoneal lymphadenopathy, and gallbladder hydrops with minimal biliary sludge (Images D and E). UPCH Case Editors: Carlos Seas, Course Director / Paola Nakazaki, Associate Coordinator |
|
  Discussion: KOH examination of an induced sputum sample (Image F) revealed large, oval, double-walled yeast cells with multiple budding daughter cells, characteristic of Paracoccidioides species. Our patient underwent ERCP, during which a biliary sphincterotomy with balloon sweep was performed, and a biliary stent was placed. Nodular erosive lesions were observed in the duodenum, and a biopsy was obtained. Histopathologic evaluation of duodenal mucosa reported glandular architectural changes and moderate chronic inflammation with the presence of yeasts; no granulomas were reported (Image G), and a lymph node biopsy (Image H) demonstrated a mixed necrotizing granulomatous inflammatory process with abundant yeast-like fungal structures of variable size on hematoxylin and eosin staining. Paracoccidioidomycosis is an endemic mycosis caused by fungi of the genus Paracoccidioides, predominantly Paracoccidioides brasiliensis. It primarily affects rural populations in Latin America, particularly in tropical regions such as Brazil, Peru, Venezuela, Ecuador, and Colombia (1). It is strongly associated with agricultural work, where exposure to soil is important. Paracoccidioides species reside in the environment in their mycelial form and are acquired through inhalation; once inside the host, the fungus undergoes thermal dimorphism, transforming into its yeast form (2). Paracoccidioidomycosis presents with diverse clinical manifestations and is generally categorized into two main forms: the acute/subacute (juvenile) form and the chronic (adult) form. In severely immunocompromised patients, it may present with features of both forms (3). The juvenile form is the least common, occurring in 5% to 25% of cases, and it primarily affects children and young adults under 35 years, with equal gender distribution. It progresses rapidly, typically presenting with fever, weight loss, and generalized lymphadenopathy. Hepatosplenomegaly, abdominal symptoms, skin lesions, and, occasionally, bone involvement may occur, while pulmonary involvement is uncommon (2,3). The chronic form accounts for 75% to 95% of cases and typically affects men aged 30 to 60 years. It has a slow onset and may be localized or disseminated. Pulmonary involvement is most common, presenting with chronic respiratory symptoms and weight loss. Mucocutaneous oral lesions are frequent, and adrenal involvement may occur. Fever and significant lymphadenopathy are uncommon (2,3). Although our patient is outside the typical age range for the juvenile form, he meets clinical criteria consistent with this presentation. Additionally, high-dose corticosteroids may have contributed to accelerated clinical progression. Paracoccidioidomycosis is diagnosed by demonstrating P. brasiliensis in clinical specimens. The fungus can be identified by direct microscopy of sputum, skin scrapings, or biopsy material, including tissue sections stained with hematoxylin and eosin or Gomori–Grocott. Serologic assays for antibodies or antigens may support the diagnosis, although their sensitivity varies and cross-reactivity with other endemic mycoses can occur. Additional diagnostic tools include PCR techniques and fungal culture (4). All patients with the juvenile form should receive amphotericin B. The deoxycholate formulation is administered at 0.5–0.7 mg/kg/day (maximum 50 mg/day). Once clinical stabilization is achieved, the regimen is transitioned to an oral azole derivative or trimethoprim–sulfamethoxazole (3, 5). Our patient is currently receiving amphotericin B and is showing clinical and laboratory improvement, with a significant decrease in previously elevated liver function tests. References |