 |
Gorgas Case 2026-7 |
|
The following patient was seen on the inpatient ward of Cayetano Heredia Hospital in Lima by the 2026 Gorgas Course participants.
 History: A 49-year-old woman presents with a six-month history of progressively enlarging nodular skin lesions. About one month after sustaining a wound on her finger while preparing fish, she noticed a non-painful, non-pruritic spot and a nodular lesion at the injury site. Over the following months, the lesion persisted, and additional nodular lesions appeared, extending along a lymphatic tract from the original site. She denies fever or other systemic symptoms. Epidemiology: The patient was born and currently lives in a rural area of the Peruvian highlands, in San Ignacio, Cajamarca, at about 1,324 meters above sea level. She works in agriculture and gardening on her own farm, which involves frequent contact with soil and plant material. She denies close contact with people who have similar lesions. Physical examination: HR: 74, RR: 18, T: 36.7°C, BP: 120/70, SatO2: 98% on room air. On physical exam, a primary lesion is seen on the finger at the initial injury site (Image A). Additional nodular lesions are present along the lymphatic vessels extending proximally from the primary lesion (Images B, C). They are not associated with warmth, pruritus, or tenderness. The rest of the physical exam is unremarkable and noncontributory.. Laboratory: Initial tests revealed hemoglobin at 15.1 g/dL and leukocytes at 4160, with 52.1% neutrophils, 39.7% lymphocytes, 0.2% basophils, 6.3% monocytes, and 1.7% eosinophils. Platelet count was 158000. Liver function tests revealed AST at 27.5 U/L (normal range 8 to 48 U/L) and ALT at 18.60 U/L (Normal range 7 to 55 U/L). Total bilirubin was 0.46 mg/dL, with direct bilirubin at 0.19. UPCH Case Editors: Carlos Seas, Course Director / Paola Nakazaki, Associate Coordinator |
|
 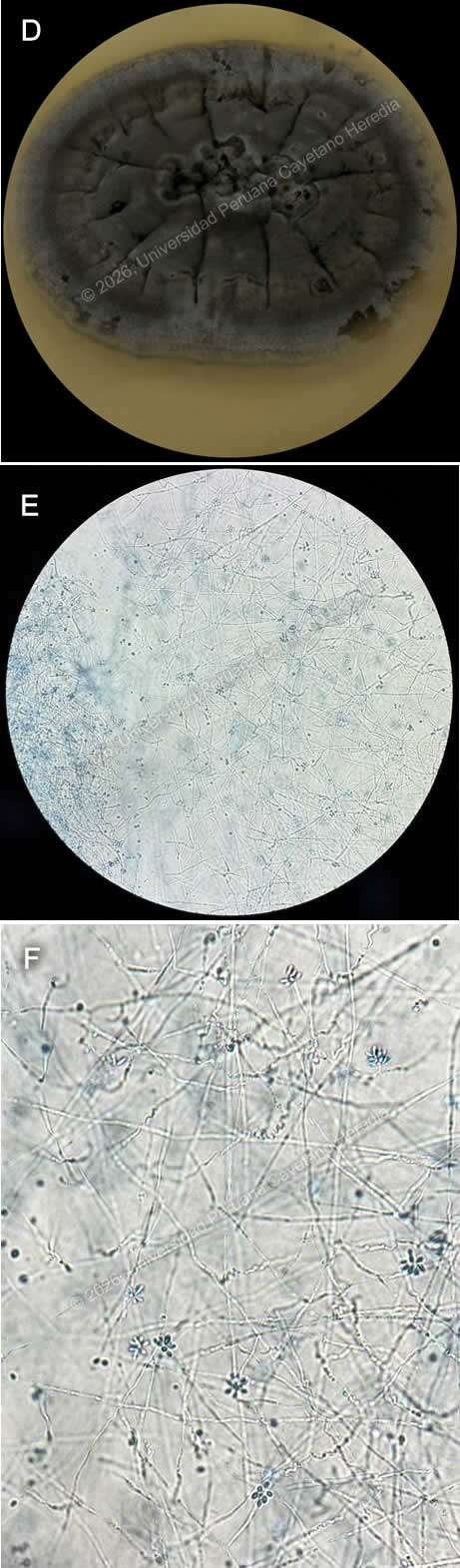 Discussion: A biopsy from the lesion was taken, direct observation was negative for Leishmania, blood agar culture for Leishmaniasis was negative as well. Culture for common germs and MGIT for Mycobacteria were negative. Agar Sabouraud fungal culture was positive for Sporothrix spp., confirming the diagnosis (Image D). Direct microscopic observation from the culture revealed thin hyphae, from which small, oval conidia arise, and often cluster in a “rosette” or “daisy-like” pattern, a feature suggestive of the genus Sporothrix (Images E, F). Sporotrichosis is a subcutaneous mycosis caused by dimorphic fungi of the genus Sporothrix, most commonly Sporothrix schenckii. It is found worldwide but is most prevalent in tropical and subtropical regions. It is frequently identified in Central and South America, the southern United States, Africa, and Southeast Asia, with recognized hyperendemic areas such as Guatemala, Mexico, Peru, and South Africa (1). In Peru, highland regions are considered endemic, with most cases reported from Abancay and Cajamarca (2). It is frequently associated with farming and gardening activities, existing as its mycelial or filamentous form in soil, wood, plant debris, and organic matter at lower temperatures around 25°C. In the human body, it transforms into yeast. Infection occurs when the organism is introduced into the skin through traumatic inoculation of the fungi (3). Clinical presentation may vary; it most frequently manifests as fixed cutaneous or lymphocutaneous, beginning with a lesion at the site of inoculation, followed by secondary lesions along lymphatic tracts. Rarely does it spread via the hematogenous route, leading to the disseminated form, which may present with organ involvement and multiple skin lesions at noncontiguous sites, and is associated with immunocompromised hosts (3,4). Diagnosis can be challenging because its clinical manifestations may resemble other conditions, such as cutaneous leishmaniasis, nocardiosis, tularemia, infections by atypical mycobacteria, and cutaneous tuberculosis. Therefore, diagnosis relies on a combination of clinical history, exposure, epidemiological context, and physical examination findings; it is supported by laboratory confirmation, with fungal culture being the gold standard. Other methods include direct microscopy, histopathology, and PCR to assist in identifying species (5,6). Management varies according to the clinical presentation and severity of the disease. Oral itraconazole is the treatment of choice for cutaneous and lymphocutaneous sporotrichosis and is typically continued for one month after complete clinical resolution is achieved. In more severe or disseminated forms of the infection, initial therapy is indicated with amphotericin B, followed by oral itraconazole (4,5). Our patient had the lymphocutaneous presentation and received Itraconazole; she is currently in her third month of treatment with no adverse events. References |