 |
Gorgas Case 2026-8 |
|
The following patient was seen on the inpatient ward of Cayetano Heredia Hospital in Lima by the 2026 Gorgas Course participants.
 History: The patient is a 41-year-old man from Lima who presents with a 6-month history of a progressive illness characterized by a pruritic maculopapular rash initially involving the arms and legs, which evolved into plaques with fine desquamation. This has been accompanied by intermittent fever and generalized malaise. Over the same period, he reports chronic watery diarrhea (5–6 episodes daily), including two episodes of bloody diarrhea, associated with anorexia, abdominal bloating, and unintentional weight loss of 14 kg. He also notes the development of whitish oral plaques and dysphagia to solid foods. He denies vomiting, seizures, loss of consciousness, cough, dyspnea, and night sweats. Epidemiology: The patient lives in Rimac, an urban area of Lima, where he works as a construction worker. He reports a history of alcohol use on weekends since adolescence, which he stopped 10 years ago. Currently, he smokes about one cigarette per week and uses marijuana. He also has a history of multiple female sexual partners (exact number unknown) with inconsistent condom use. Additionally, he previously had gonorrhea in 2010 and completed treatment for it. Physical examination: HR 76, RR 16, Temp 36.8°C, BP 120/70, SpO₂ 97% on room air. The patient appears with dry skin and mild pallor. Dermatologic examination shows plaque-like lesions mainly on the neck, arms, and legs, as well as hyperpigmented, scaly patches on the abdomen, back, palms, and soles (Images A,B,C,D). There is significant scaling of the scalp and eyebrows. Hair is sparse and brittle, with areas of alopecia (Image E). Palpation reveals non-tender lymphadenopathy in both inguinal regions. Genital exam shows erosive lesions on the penis with mild swelling and tenderness, along with whitish discharge at the balanopreputial sulcus; no ulcers are present. Neurological assessment indicates the patient is alert and oriented, with no focal deficits or meningeal signs. The remaining exam was unremarkable. Laboratory: Initial tests showed hemoglobin at 8.1 g/dL and leukocytes at 2500, with 64% neutrophils, 13.2% lymphocytes, 0.5% basophils, 10.4% monocytes, and 11.9% eosinophils. Platelet count was 291000. Total bilirubin was 0.5 mg/dL, alkaline phosphatase was 104, GGT was 35, and electrolytes and renal function were normal. An HIV test was positive, CD4 count was 35, viral load was 267000, and the HTLV-1 test was positive. A serum CrAg was positive. TB LAM was negative. Sputum GeneXpert Ultra was negative. A lumbar puncture was performed, revealing clear fluid with an opening pressure of 16 cmH2O. CSF analysis showed 2 leukocytes, 1 RBC, glucose at 46, capillary glucose at 180, and protein at 74. No organisms were seen on Gram stain, GeneXpert Ultra from the CSF was negative, LFA for cryptococcosis was negative in both blood and CSF, and Indian ink was negative. VDRL in CSF was negative. UPCH Case Editors: Carlos Seas, Course Director / Paola Nakazaki, Associate Coordinator |
|
 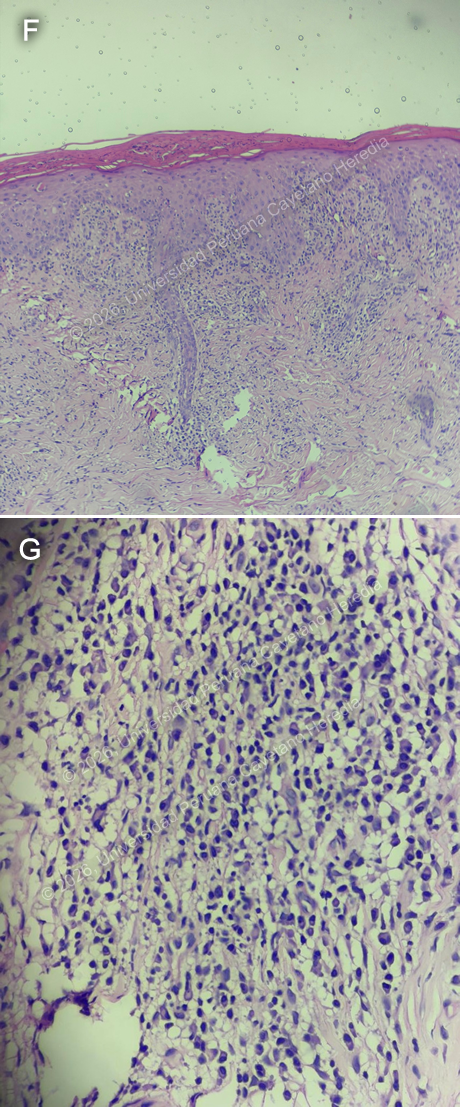 Discussion: The initial RPR was negative, but repeat testing after a prozone effect showed 1:512 dilutions. A skin punch biopsy from lesions on the right arm shows that the stratum corneum exhibits signs of parakeratosis. In contrast, the epidermis displays moderate acanthosis with lymphocyte exocytosis and occasional apoptotic keratinocytes (Image F). The dermis reveals a moderate inflammatory infiltrate composed of lymphocytes and plasma cells (Image G), distributed around skin appendages and involving both superficial and deep layers, along with some extravasated red blood cells and dilated blood vessels. Overall, these histological findings, when correlated with the clinical context, are consistent with secondary syphilis. Dark-field microscopy was not available. Syphilis is a preventable and curable infection caused by Treponema pallidum, transmitted mainly through sexual contact, but also vertically and via blood products, with increasing incidence worldwide (1). The latest data from the WHO indicates that an estimated 8 million adults aged 15 to 49 contracted syphilis in 2022. Co-infection between syphilis and HIV is common, as they share transmission routes and risk factors (2). HIV and HTLV are closely related retroviruses with similar structures, target cells, and transmission routes. As a result, coinfection is common in endemic regions; studies in the Peruvian Amazon have reported up to 10% prevalence of HIV and HTLV-1/2 coinfection (3). This is clinically significant because the interaction between these viruses can influence disease progression; patients can develop AIDS more rapidly and face higher mortality rates. HTLV-1 is also associated with immune system disruption, affecting the normal function of CD4+ and CD8+ T cells, which can weaken immune defenses and increase vulnerability to opportunistic infections (4). Syphilis presents with primary, secondary, latent, and tertiary stages. Secondary syphilis is the systemic phase that usually develops after hematogenous and lymphatic spread of the organism from the initial site of infection. It can occur weeks to a few months after the primary stage and may involve multiple organ systems. It is also highly infectious (2,5). Secondary syphilis is known for its wide range of clinical presentations, earning it the nickname the “great imitator.” It is characterized by diffuse skin lesions, often involving the palms and soles. Its presentation can vary in patients with HIV and may include other forms such as plaques, nodular lesions, painful target lesions, and pustular ulcers. Mucocutaneous lesions and lymphadenopathy may also be present. Additional manifestations can include patchy alopecia and, less commonly, organ involvement and systemic symptoms (6,7). Diagnosis is primarily based on serologic testing guided by clinical suspicion. Nontreponemal tests are used for screening and monitoring, with positive results confirmed by treponemal-specific assays. Direct detection methods such as dark-field microscopy or PCR may be used in select cases but are not routine practice (7). Treatment of choice for secondary syphilis is a single intramuscular dose of benzathine penicillin G. For patients with a penicillin allergy, alternatives such as doxycycline or ceftriaxone may be considered. After therapy, patients should be observed for the Jarisch–Herxheimer reaction. Follow-up with serial nontreponemal titers is recommended to ensure an adequate response to treatment. Tests are recommended at 3, 6, and, when indicated, 12 months post-treatment. A fourfold reduction in RPR titer or conversion to a non-reactive result indicates successful therapy (7,8). Our patient received treatment, under suspicion of possible neurologic involvement, with intravenous sodium penicillin for fourteen days, followed by a single intramuscular dose of penicillin G, with no adverse events. He also received treatment with fluconazole because of a positive serum cryptococcal antigen. And was started on prophylaxis with trimetoprim-sulfametoxazole. After ruling out other pathologies, he was started on antiretroviral therapy. References |