| 2004 Case #3 |  |
|
| The patient was seen by the Gorgas Course participants in the Opthalmology Department of the Tropical Medicine Institute. We are grateful to Dr. Isais Rolando, Professor of Opthalmology at UPCH, Associate Investigator of the Tropical Medicine Institute, and Gorgas Course ophthalmology consultant for the retinal images and his expert advice on diagnosis and management of this case. |
 History: 28 yo male with no previous medical history with 9 months of progressive loss of visual acuity in the left eye and 4 months of similar visual loss in the right eye. No pain, photophobia, headache, or ocular discharge. No history of fever or rash. No history of TB, STDs. History: 28 yo male with no previous medical history with 9 months of progressive loss of visual acuity in the left eye and 4 months of similar visual loss in the right eye. No pain, photophobia, headache, or ocular discharge. No history of fever or rash. No history of TB, STDs.
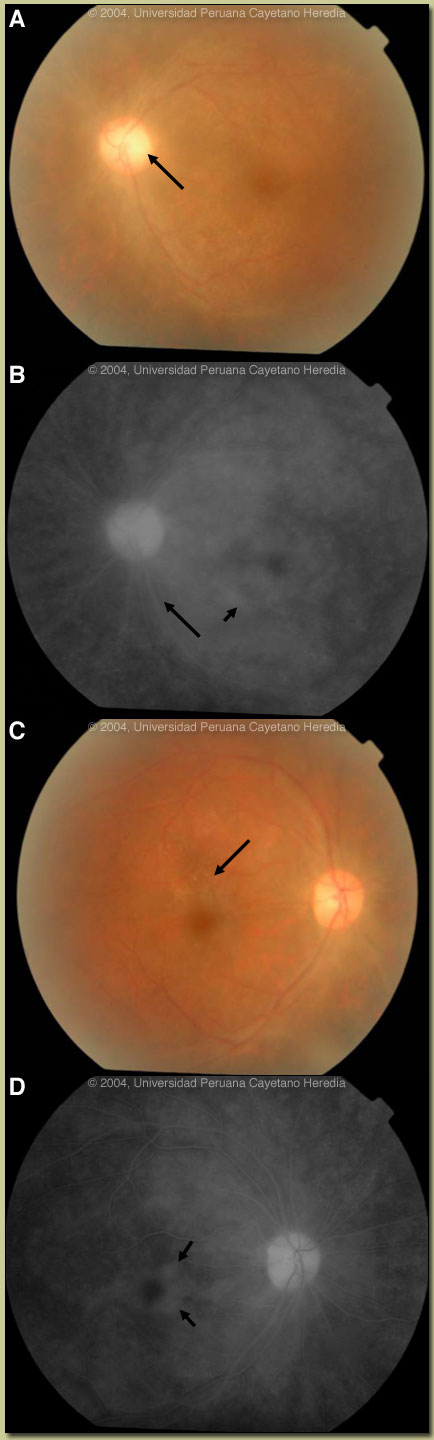
Epidemiology: Born and lives in Lima. States he has been monogamous with the same female partner for the last 4 years. Immediately prior had one female partner known to have been promiscuous. Physical Examination: Afebrile without rash, splenomegaly or lymphadenopathy. Normal neurological examination. Abnormalities restricted to the ocular examination. L eye 20/70; R eye 20/30. Bilateral vitritis on fundoscopy. Slit lamp examination — mild iritis indicated by cells in the anterior chamber bilaterally. Retina L eye with paleness of the optic disc temporally (arrow, image A). Fluorescein angiography L eye shows retinal edema, perimacular exudates, and the arrow indicates vasculitis (see image B). Retina R eye shows perimacular exudates (arrow, image C). Fluorescein angiography R eye shows retinal edema with perimacular exudates (see image D). Laboratory Examination: Hct. 32%. WBC 13.9 with 90 neutrophils and 9 lymphs. CXR normal. CSF fluid clear with opening pressure 10 mm Hg with 1 cell (100% lymphs), glucose 53 mg/dl and protein 47 mg/dl.
|
| Diagnosis: Subclinical neurosyphilis with pan-uveitis. |
| Discussion: Serum VDRL 1:64. FTA-Abs positive. CSF VDRL 1:2. Serum and CSF cryptococcal antigen negative. Brucella and salmonella agglutination negative. CSF gram stain and acid-fast negative. HIV ELISA positive with CD4 count of 145.
The differential diagnosis of infectious uveitis in a tropical environment such as ours includes most commonly tuberculosis and brucellosis, with bartonellosis and histoplasmosis being less common. This is the 3rd such case of uveitis due to syphilis in the setting of HIV we have seen in the past 12 months. In the pre-AIDS era, ocular syphilis was described as presenting either as a panuveitis as a manifestation of secondary syphilis (syphilitic meningitis), or as a manifestation of tertiary syphilis with optic neuritis, retinal degeneration, or Argyll-Robertson pupil. These latter changes were irreversible in the pre-antibiotic era. Uveitis is defined as acute (symptoms <3 months) or chronic (symptoms >3 months or insidious/indeterminant). With the appearance of AIDS, syphilis has begun to appear with clear-cut neurologic involvement earlier in its course (Clin Infect Dis 2001;32:1661-73). It is increasingly clear that syphilis patients who present initially with an isolated chronic posterior or pan-uveitis, especially in the setting of HIV (which is present in more than half these individuals), have this as a manifestation of what is demonstrably neurosyphilis. Our patient had predominantly posterior uveitis but the mild iritis means that this is a pan-uveitis. Those with acute uveitis (<3 months) generally have early or secondary syphilis but most of those with HIV co-infection have concomitant neurosyphilis. Important questions still remain about the current disease spectrum of ocular syphilis and its relationship with neurosyphilis. Nevertheless, because of the frequent association of syphilitic posterior uveitis or pan-uveitis with sub-clinical neurosyphilis, current CDC and international guidelines indicate that all such patients, irrespective of ocular disease intensity should be given a full course of treatment for neurosyphilis. In addition to direct effect on the eye disease, the other goal of therapy would be to prevent the development of symptomatic neurosyphilis. Our patient was treated intravenously for 2 weeks with 18 million IU of Penicillin G per day as well as with Prednisone 50 mg/day. At the end of treatment visual acuity in the L eye improved to 20/50 and in the R eye to 20/25. The paleness of the optic disk temporally persisted and this optic atrophy is a typical sequelae of syphilitic neuritis.
|