 |
Gorgas Case 2015-05 |
 |
|
This past week, the field trip to Cusco, Perú in the Andean highlands took place. Cusco (elevation 3,400 meters) is the oldest continuously inhabited city in the Americas. The following patient was seen in the outpatient clinic of the Cusco Regional Hospital.
 History: 54-year-old previously healthy female presents with 2 months of epigastric and right upper quadrant dull pain. The pain waxed and waned, sometimes reaching 10 out of 10, and radiated to the back. She had severe fatigue and anorexia, as well as weight loss of about 10 pounds. No fever, rash, jaundice, diarrhea, vomiting, or joint pain. She has a remote history of angioedema with 3 episodes requiring hospital admission. The patient has BRCA2 gene mutations and has undergone bilateral mastectomies and salpingo-oophorectomies in the past. Lives alone, no ill contacts.
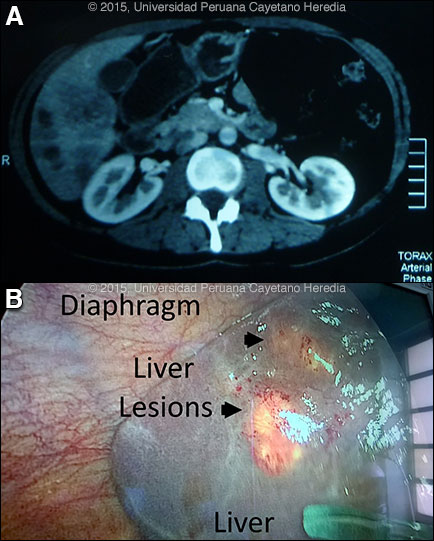
Epidemiology: Physician, born on the coast of Perú but living for many years in the suburbs of Cusco with occasional exposure to farm animals. Non-smoker, no alcohol abuse, no known TB exposures. No HIV risk factors. Normal diet without ingestion of undercooked or unusual foods. Physical Examination: Afebrile with normal vital signs. Unexceptional physical examination except for mild tenderness to palpation in the right upper quadrant of the abdomen and a palpable liver. Laboratory Examination: Altitude adjusted hemoglobin 9.9 g/dL. WBC: 12,300 with 67% eosinophils, Platelets: 387,000. AST: 38 U/L (N), ALT: 28 U/L (N). Alkaline phosphatase: 236 U/L (N<104). Total bilirubin: 1.2 mg/dL. HBsAg: Negative. HCV ab: Negative. Stool O & P negative X3. CT of the liver showed several hypodense lesions in the liver parenchyma [Image A]. The patient underwent laparascopic liver biopsy for suspected metastatic liver lesions [Image B].
|
|
Diagnosis: Fasciola hepatica infection, acute phase.
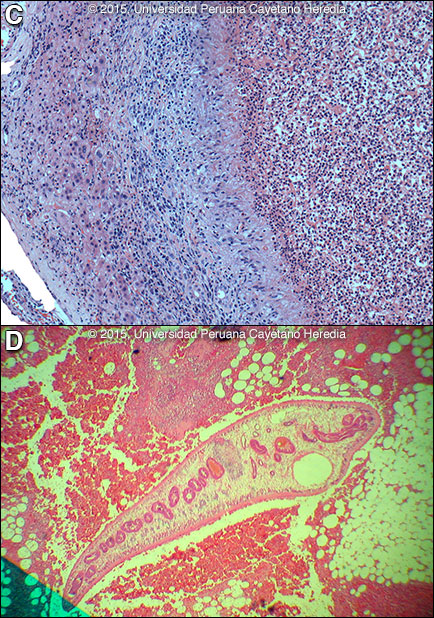
Discussion: IgG Fas2 ELISA [Trans R Soc Trop Med Hyg. 1999 Jan-Feb;93(1):54-7] was positive for Fasciola hepatica at the UPCH–UTMB (University of Texas Medical Branch Galveston) Collaborative Research Center in Cusco. This test is more specific than Western blot or Arc2 immunodiffusion. An ELISA performed 1 month earlier was negative. The liver biopsy showed eosinophilic granulomas [Image C]. A F. hepatica larva from another patient with acute infection from our case files is shown in Image D. Fasciola hepatica is a trematode (fluke or flatworm) in which the mature adult parasites inhabit the large biliary ducts. As with all other trematodes, Fasciola hepatica requires a snail intermediate host. Eggs produced by the hermaphroditic adults pass with the feces and hatch, releasing larvae in fresh water. After passing through a snail, mature cercariae emerge and rapidly encyst on various kinds of aquatic vegetation such as watercress or alfalfa. Recent data, however, also suggests waterborne transmission. Our patient denies ingestion of watercress or alfalfa, but did admit to eating salads with lettuce. After ingestion by a human or animal definitive host, the metacercariae excyst in the duodenum and larvae penetrate the intestinal wall and subsequently migrate directly into the liver via Glisson’s capsule and embark on a destructive migratory process through the hepatic parenchyma for 3 to 4 months until they reach large biliary ducts, where they then mature to adults. The mature adults are from 1 to 3 cm long and attach to the biliary epithelium by a single ventral sucker. In the absence of direct visualization of adults, characteristic eggs can be seen on stool examination, but more often patients present in the early migratory phases of infection prior to maturation of the worm and the onset of egg-laying. Specific serology is the test of choice. The distribution of F. hepatica is cosmopolitan, but is by far the most common in cattle-raising areas where herbivores are common definitive hosts. Other important definitive hosts are goats, sheep, horses, llamas, vicunas, and camels. The contiguous Altiplano regions of the Peruvian and Bolivian Andes are highly endemic, with human prevalence rates as high as 67% in some villages. In the agricultural areas near Cusco, the prevalence in children 3 to 12 years old is 11% by stool microscopy and Fas2 ELISA [Am J Trop Med Hyg. 2014 Nov;91(5):989-93]. Egypt, Cuba, and Northern Iran are also highly endemic and the parasite is emerging in Vietnam and Cambodia. Cooking, which would kill the metacercariae, dramatically changes the flavor of watercress and the population is reluctant to adopt this simple measure. Emoliente, a local tea-like drink that uses drops of watercress juice to provide a bitter flavor is a frequent vehicle of infection. Clinically, the disease can be divided into acute and chronic phases. During the acute phase, migrating parenchymal larvae generally cause fever, eosinophilia, right upper quadrant pain and especially significant anorexia. Vomiting and weight loss of 20 kg or more may develop, which usually abates when the larvae mature to adults. The adult flukes in the biliary tree are generally asymptomatic but some patients develop chronic manifestations including right upper quadrant pain, nausea, vomiting, and hepatomegaly. Eosinophilia and abnormal liver function may develop but are less common than with acute disease. Adult flukes may cause hyperplasia, desquamation, thickening, and dilatation of the bile ducts. Malignant degeneration and cholangiocarcinoma such as results from chronic infection with the oriental liver fluke Clonorchis sinensis has not been reported with F. hepatica. We have reported a case series with clinical findings and evolution of disease [Am J Trop Med Hyg. 2008 Feb;78(2):222-7]. Please see Gorgas Case 2005-02 for a CT image of another example with the typical larval tracks seen in acute disease. The differential diagnosis of eosinophilia with accompanying destructive hepatic lesions is limited. Toxocariasis causes hypereosinophilia with hepatomegaly but the pathology results from small granulomas around individual non-migrating larvae and not the large destructive lesions seen in our patient. Eosinophilia is common in Perú, so it may be due to an unrelated event present concomitantly with a bacterial liver abscess; this had been the initial impression in this case. Fasciola hepatica is the only trematode infection for which praziquantel is not the drug of choice. The WHO has put the anthelmintic triclabendazole (Egaten, Novartis) on its essential drugs list. Egaten is registered in Perú (as in Mexico and Egypt) and is available via free donation from the WHO. In the U.S. the drug is available from the CDC Parasitic Drug Service. The usual dosage is 10 mg/kg with a meal. Many practitioners repeat the dosage 12 to 24 hours later. In intial studies at our institute the cure rate was 96%, but it has been lower in recent experience. Treatment with triclabendazole 10 mg/kg in a single dose was provided to the patient with resolution of her symptoms within one week. On follow up 6 weeks after treatment, she has recovered her appetite and energy level and her altitude adjusted hemoglobin level is 11.4 g/dL.
|