
The prevalence of kidney stones is significantly increasing in the United Sates.
An analysis of the National Health and Nutrition Examination Survey (NHANES) data demonstrated that the prevalence of kidney stones in the U.S. from 1988 to 1994 was 5.2% and this skyrocketed to 8.8% from 2007 to 2010.
Economic Impact
This increase is associated with a tremendous economic burden. Saigal and associates as part of the Urological Disease in America Project reported that 1% of employed Americans had a kidney stone event in 2000, 30% having to miss work. They estimated that the mean time away from employment was 19 hours. The direct costs for patient management were estimated to be 4.5 billion dollars and indirect costs due to being away from the labor force was 775 million dollars. Thus, the estimated economic burden for 2000 approached 5.3 billion dollars. Factoring in the costs of providing care for those not in the labor force, the rising prevalence of kidney stones and inflation, today’s yearly costs for providing kidney stone care in the United States would be substantially more. Kidney stones also have a negative impact on quality of life. The detrimental impact of quality of life can even extend to those with asymptomatic stones. Given the aforementioned negative factors associated with kidney stones, new knowledge regarding mechanisms of stone formation is highly relevant and could lead to novel therapies.
Obesity
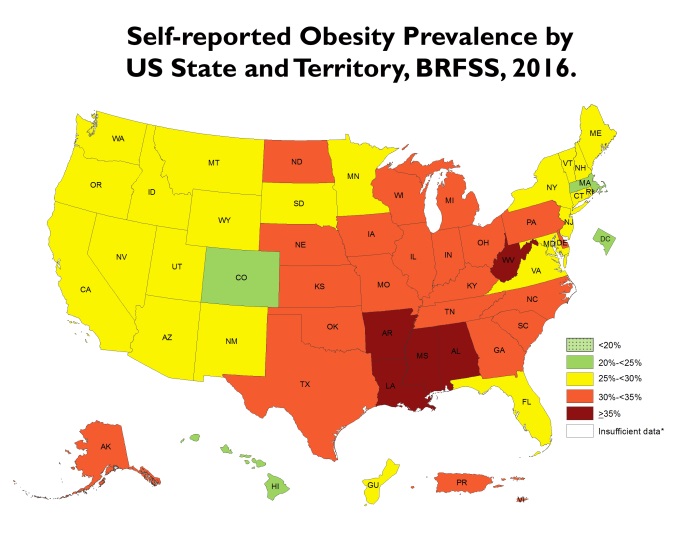 Figure 1. Prevalence of Self-Reported Obesity Among U.S. Adults By State and Territory, Behavioral Risk Factor Surveillance System, 2016. *sample size <50 or the relative standard error (dividing the standard error by the prevalence) >30%The prevalence of obesity is also increasing in the United States. The most recent report from the Center for Disease Control (CDC) indicated that the prevalence of obesity in adults in the United States is now 36.5% (https://www.cdc.gov/obesity/data/prevalence-maps.html). An obesity map provided by the CDC demonstrates that the Southeastern part of the United States is a hotbed, and Alabama is one of the five states with the highest prevalence (Figure 1).
Figure 1. Prevalence of Self-Reported Obesity Among U.S. Adults By State and Territory, Behavioral Risk Factor Surveillance System, 2016. *sample size <50 or the relative standard error (dividing the standard error by the prevalence) >30%The prevalence of obesity is also increasing in the United States. The most recent report from the Center for Disease Control (CDC) indicated that the prevalence of obesity in adults in the United States is now 36.5% (https://www.cdc.gov/obesity/data/prevalence-maps.html). An obesity map provided by the CDC demonstrates that the Southeastern part of the United States is a hotbed, and Alabama is one of the five states with the highest prevalence (Figure 1).
Kidney Stone Belt
Interestingly, the Southeast is considered to be the kidney stone belt, a region of the country where there is the highest prevalence of kidney stone formers (Figure 2). There is ample evidence that obesity is linked to kidney stone risk. In a study of three large epidemiologic cohorts (Nurses’ Health Study I, Nurses’ Health Study II, Health Care Professional Follow-up Study), Taylor and associates found that both body mass index (BMI) and waist circumference, two measures of obesity, were positively correlated with the risk of developing an incident kidney stone. In an analysis of the Women's Health Initiative Observational Study, a cohort of 84,225 women with no history of kidney stones, Sorensen and colleagues identified a BMI dependent increased risk of incident kidney stones, 25-29.9 kg/m2 (1.3 fold ), 30-34.9 kg/m2 (1.62 fold ), and ≥ 35 kg/m2 (1.81 fold ) as compared to BMI < 25 kg/m2. This rise in obesity, if it continues unabated, is predicted to directly increase the prevalence of kidney stones in 2030 by 0.36% resulting in over a billion more dollars of health care costs. COOKS is ideally situated to conduct the proposed research. 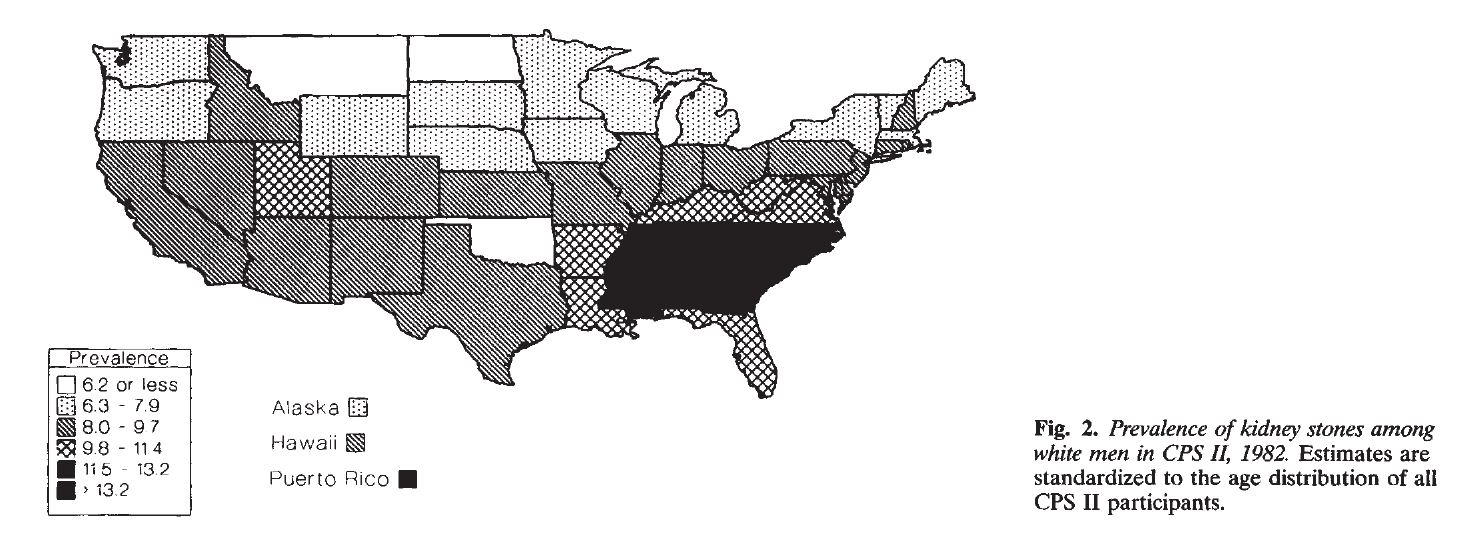
Additional Research is Needed
While the associations between obesity and kidney stone risk have been defined, the mechanisms behind this relationship warrant further investigation.
Calcium oxalate is the most common stone composition including in obese subjects. Numerous factors are involved in the generation of such stones including the amount of oxalate excreted in urine. This has notably been reported by Curhan and associates in the analysis of Nurses’ Health Study I, Nurses’ Health Study II, Health Care Professional Follow-up Study, where Curhan and associates found a high positive correlation between urinary oxalate excretion and the risk of developing a kidney stone. Obese kidney stone formers most commonly form calcium oxalate stones as do non-obese individuals, and their urinary oxalate excretion has been shown to be higher than that of individuals without obesity in several published studies. In their study, Lemann and associates reported a highly significant positive correlation between urinary oxalate excretion, body weight, body surface area and urinary creatinine in healthy non-stone forming adults and hypothesized that this was due to increased endogenous oxalate synthesis as body mass increased. Urinary oxalate is derived almost equally from diet and endogenous oxalate synthesis, the latter occurring in the liver. It cannot be determined what the cause is for the increase in urinary oxalate excretion in the obese cohort from the aforementioned studies.
There is a definite paucity of information regarding the influence of systemic conditions such as obesity on the production of oxalate. Hence, the proposed investigations would advance urological research and have a profound impact on the benign urological disease research community. This project will advance urological research by providing more knowledge regarding an important factor contributing to kidney stone formation in an at risk population, those with obesity. Alabama is a state where both conditions are common, being a part of both the “obesity and stone belts” of the United States. Thus, this research has definite public health relevance and significance, especially for the Southeastern part of the United States.