| 2009 Case #11 |  |
|
|
We hope you have enjoyed the 2009 series of live cases each week from Perú. The Gorgas Diploma Course runs annually in February and March and we will be in touch at the beginning of next year’s case series. In addition to the 2009 cases on the Gorgas website, cases from previous years are available for full CME credit at no charge at the UAB School of Medicine's Division of Continuing Medical Education. Eduardo Gotuzzo, M.D. and David O. Freedman, M.D. |
| The following patient was seen by Gorgas Course participants in the outpatient department of the Tropical Medicine Institute. We thank Gorgas Course Dermatology Professor Dr. Francisco Bravo for consultation on the case and in interpretation of the pathologic specimens. |
|
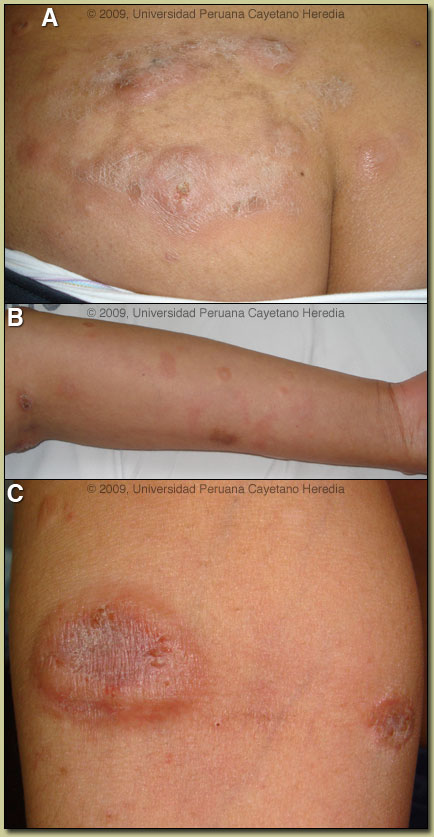
Epidemiology: Born and lives in Lima. Psychologist. Unmarried. No HIV risk factors. No history of travel to jungle or highland areas. No apparent TB exposures. Physical Examination: Afebrile. Normal general appearance. Chest clear. No hepatosplenomegaly or lympadenopathy. Normal neurological examination. Skin [see Images A, B, C]: multiple plaques and nodules, many with a raised border and depressed center. Some are scaly at the center; some with minimal exudation. The lesions are painless and highly pruritic. They are located on limbs, chest, abdomen and buttocks (where they are more confluent). Sensation is preserved over the lesions and surrounding areas. Laboratory Examination: [During initial presentation 1 year earlier.] Hb 13.5, Plt 283 000, WBC 2780, GGT 29 (normal) AST 48 (normal), ALT 43 (normal), LDH 726 (normal <300) RPR (-), Stool O & P x3 (-), all hepatitis B markers (-). HIV (-). Chest X-ray normal. Abdominal CT scan normal. |
| Diagnosis: Adult T-cell leukemia/lymphoma (ATLL), smoldering type. HTLV-1 infection. |
|
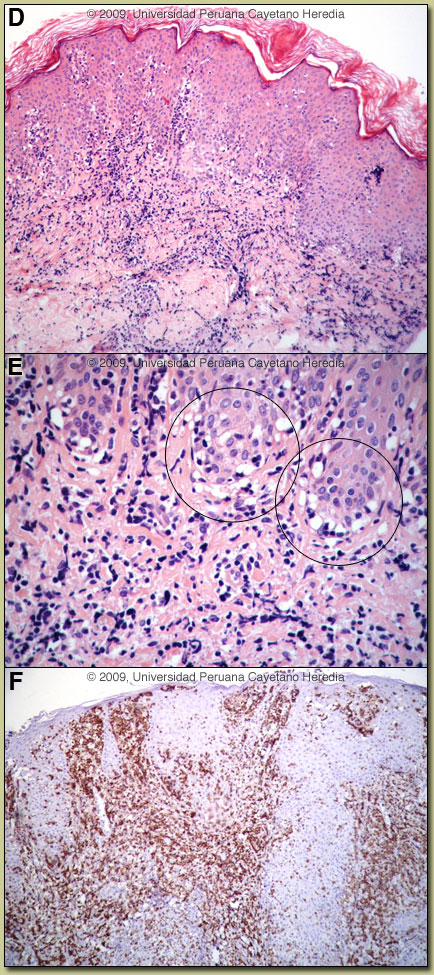
On initial clinical presentation this patient’s lesions in a tropical setting provided an unusually broad differential diagnosis even in expert hands. Possibilities include cutaneous tuberculosis, atypical mycobacteria, cutaneous manifestations of Balamuthia mandrillaris or other free-living amebas, sporotricosis, syphilis, diffuse cutaneous leishmaniasis, disseminated leishmaniasis with or without HIV co-infection, and finally leprosy. Non-infectious processes such as atypical pityriasis rosea or mycosis fungoides have to be included on the basis of clinical appearance alone. Adult T-cell leukemia/lymphoma (ATLL) due to HTLV-1 infection is sub-divided into four categories: acute, lymphomatous, chronic, and smoldering [J Clin Oncol. 2009 Jan;27(3):453-9]. The latter two types are considered indolent and may be treated with watchful waiting until disease progression or invasion. This is somewhat analogous to the situation with chronic lymphocytic leukemia (CLL). Patients with the more aggressive forms generally have a poor prognosis (survival <1 year) despite aggressive conventional chemotherapy; many different regimens have provided no measurable benefit. Aggressive forms are associated with hypercalcemia and opportunistic infections. Typical ATLL cells have multi-lobular nuclei with homogeneous and condensed chromatin, small or absent nuclei, and agranular and basophilic cytoplasm. These so-called flower cells were not seen in the biopsy and are generally not seen in the peripheral blood or skin of patients with smoldering disease. Mildly elevated LDH as in this patient is often seen in smoldering disease. Other conditions associated with HTLV-1 infection [see Lancet Infect Dis. 2007 Apr;7(4):266-81 for a detailed discussion] are tropical spastic paraparesis (TSP) also called HAM (HTLV-1 associated myelopathy) [see Gorgas Case 2002-08], disseminated strongyloidiasis, crusted (Norwegian) scabies [see Gorgas Case 2008-08], infective dermatitis [see Gorgas Case 2004-07], autoimmune disease including uveitis, Sjögrens, arthropathy, polymyositis, and thyroiditis. This patient did not have any neurological findings. More than 90% of individuals with HTLV-1 infection remain asymptomatic for life. Worldwide, approximately 0.3-4.0% develop TSP and 1-5% develop ATLL. Although the pathogenetic mechanisms of these two major complications likely differ, the low rates of each means that it is rare to see both sequelae in the same patient. The prevalence of HTLV-1 in South America is generally underappreciated, normally being associated with Japanese and Caribbean populations. HTLV-1 is now known to occur worldwide, having originated in Africa. The highest prevalence is in Japan. In Perú, the disease is highly endemic (2-3% seropositivity) in Andean areas of the country, in Quechua populations who have had no contact with Japanese immigrants to the country. Other South American countries with significant rates of HTLV-1 include Brazil, Colombia, Agentina, and Ecuador. Transmission appears to be mainly vertical with high associations with breastfeeding and duration of breastfeeding (probable route in our patient). Transfusion, sexual transmission, and IV drug abuse are much less important. The HTLV-1 induced nature of the lymphoma was not appreciated initially at the referring hospital and she received 5 courses of conventional chemotherapy with some response. Therapy was discontinued due to recurrent neutropenia and fever. The most promising intervention for aggressive disease forms has been with the use of anti-viral therapy. The combination of Zidovudine (AZT) with IFN-α [J Clin Oncol. 2009 Jan;27(3):453-9] if used as a first-line treatment dramatically increases survival in acute forms of ATLL but has no effect in lymphomatous forms. Because of her uncomfortable and disfiguring skin lesions our patient will receive a trial of AZT/IFN-α and if she responds this will be maintained indefinitely. Recent data has shown a 100% 10-year survival in smoldering ATLL treated with ongoing anti-retrovirals compared to a 42% 5-year survival in patients allowed to progress naturally and treated with chemotherapy in later stages of disease. |
 Discussion:
Discussion: