| 2009 Case #6 |  |
| The following patient was seen by the Gorgas Course participants on the 36-bed inpatient ward of the Tropical Medicine Institute. |
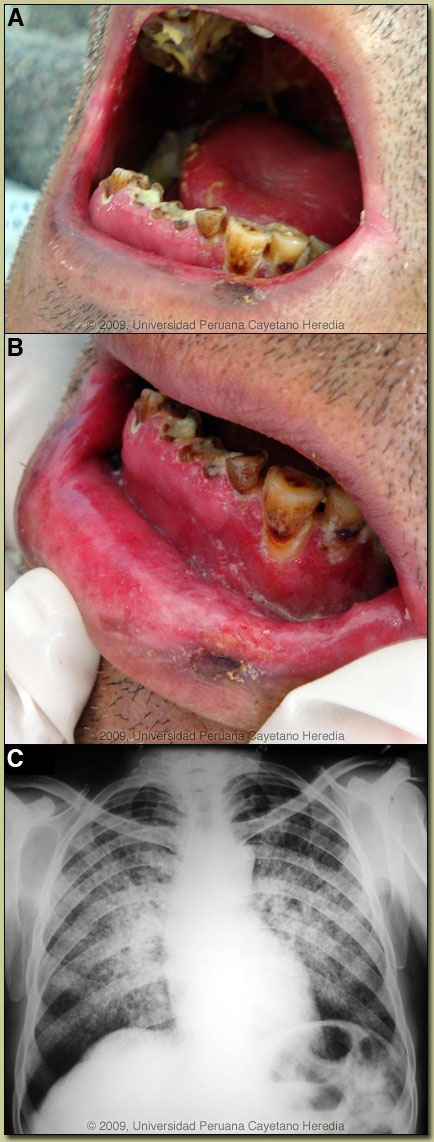
|
Epidemiology: Born in and currently works as a farmer in Ancash in the Andean highlands. Lived more than five years in the jungle regions of Huánuco in central Perú with poorly described history of an episode of malaria at that time. No history of or close contacts with TB. Physical Examination: Afebrile, HR 88, resp 26, BP 90/70. Chronically ill appearing, no skin lesions, no lymphadenopathy. Edematous gums with erythematous and granulomatous infiltration, poor dental hygiene with many missing teeth [Images A & B]. Multiple oral ulcers with erythematous infiltration. Rales bilaterally. Liver palpated 4 cm below the costal margin. No splenomegaly. Laboratory Examination: Hb 12.9; WBC 12,300 (80% PMNs, 12% lymphs), 673K platelets. Normal glucose, creatinine, bilirubin and transaminases. Albumin 2.8 (N > 3.5). Normal urinalysis. Oxygen saturation was 92% on room air. Chest x-ray is shown in Image C. |
| Diagnosis: Paracoccidioides brasiliensis infection (chronic form) with mucosal involvement. |
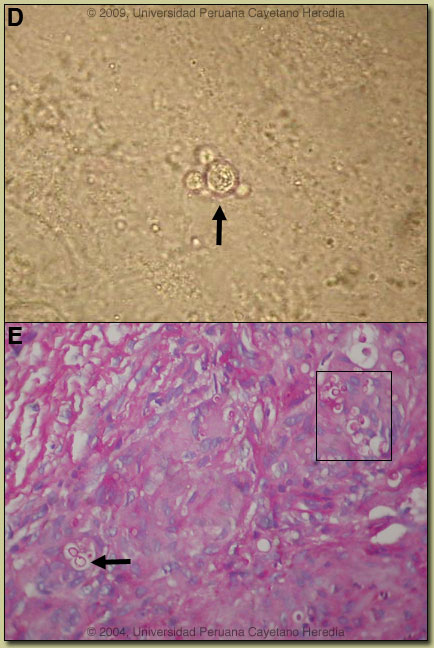 Discussion: The diagnosis was made by simple KOH preparation of a mucosal scraping, which showed typical pilot-wheel shaped organisms [Image D, arrow] consisting of spherical cells 10-40 microns in diameter with a thick birefrigent cell wall surrounded by several peripheral buds. Direct scrapings will be positive in up to 90% of cases of paracoccidioidomycosis with oral lesions. Sputum AFB stain was negative. We did not perform a biopsy but a typical lip biopsy result from a previous Gorgas Case is shown in Image E, demonstrating granulomas with multinucleated giant cells containing yeast forms of P. braziliensis (PAS stained; see arrow and boxed area in image). Discussion: The diagnosis was made by simple KOH preparation of a mucosal scraping, which showed typical pilot-wheel shaped organisms [Image D, arrow] consisting of spherical cells 10-40 microns in diameter with a thick birefrigent cell wall surrounded by several peripheral buds. Direct scrapings will be positive in up to 90% of cases of paracoccidioidomycosis with oral lesions. Sputum AFB stain was negative. We did not perform a biopsy but a typical lip biopsy result from a previous Gorgas Case is shown in Image E, demonstrating granulomas with multinucleated giant cells containing yeast forms of P. braziliensis (PAS stained; see arrow and boxed area in image).
The major differential diagnosis in Perú of oro-pharyngeal lesions in non-HIV infected patients would be mucosal leishmaniasis, paracoccidioidomycosis, carcinoma, or lymphoma. In Perú, leishmaniasis with destructive but painless lesions would be by far the most common. In general, oral lesions of paracoccidioidomycosis are painful, are frequently friable and bleed on contact, and gingival and buccal mucosa are frequently involved. The differential diagnosis for the lung disease includes: TB, histoplasmosis, lymphoma, cancer and cryptococcosis. This patient demonstrates the most typical radiographic pattern of paracoccidioidomycosis with bilateral mixed infiltrates (alveolar and interstitial), mainly located in the middle and lower lobes. Interstitial lesions may have a miliary, nodular or fibronodular patterns. Other patterns observed in these patients are hilar and mediastinal lymph node enlargement, cavities, and calcified lesions. Extrapulmonary disease is found in over 70% of cases and may involve skin, mucous membranes, lymph nodes, adrenals, abdominal organs and CNS (in 10%). Bacterial superinfection of ulcerative oral lesions when they occur is more common than with oral ulcers due to mucocutaneous leishmaniasis. This case is representative of the chronic form (adult type) of the disease, which is believed to represent reactivation of latent infection. This type represents approximately 94% of all cases in the experience at our institute (94 patients, up to 2001), and approximately 85% in the Brazilian series [Rev Soc Bras Med Trop. 2003;36(4):455-9]. In our experience the male:female ratio in chronic paracoccidioidomycosis is 20:1. TB coexists in up to 10% of patients with paracoccidioidomycosis. Cavitation and pleural effusion are less commonly seen than in TB. We have previously presented cases of two other clinical forms of paracoccidioidomycosis: (1) the juvenile form [Gorgas Case 2006-02]; and (2) the chronic progressive form [Gorgas Case 2003-07]. Paracoccidioidomycosis, also known as South American blastomycosis, is found in humid forested or lush green areas of the Americas from Southern Mexico south to Uruguay and Argentina. It appears to be most common in Brazil. The exact habitat of the organism is unclear but transmission is described as being entirely by airborne inhalation. However, we have observed cases with only oral lesions apparently associated with the use of tree leaves contaminated with fungal spores as toothpicks. Primary pulmonary infection may be asymptomatic and self-limited, but even with treatment, will produce at least moderate pulmonary fibrosis. Rural adult male agricultural workers between 30-60 years of age are most affected by the infection. Travelers spending less than 6 months in an endemic area are unlikely to acquire paracoccidioidomycosis. Sulfonamides, ketoconazole, itraconazole, and amphotericin B are all effective therapies. Amphotericin should be reserved for severe cases such as this one where there is some respiratory compromise. For typical cases, itraconazole 100-200 mg/day for 6-9 months is regarded as the treatment of choice when it is available and affordable. Relapses are common with less than 6 months therapy and expert opinion is now that 1 year is not necessary. In the developing-world setting, ketoconazole is likely equally effective and is usually less than half the cost. However, 12 months of therapy with ketoconazole is generally recommended. In severe cases with a high yeast burden, such as in our case, the practice is to induce such patients with amphotericin B for at least 10 days at 1 mg/kg, then switch to oral itraconazole 200 mg per day, to complete a total duration of at least 9 months. |