2006 Case #2 |
 |
| The following patient was seen by course participants on the 36-bed Tropical Disease Unit at UPCH. |
 History: 46 yo male admitted with a 2-month history of low grade fever, weight loss (5kg), productive cough the first two weeks, epigastric pain and diarrhea. 2-3 loose stools per day for the first 3 weeks. History: 46 yo male admitted with a 2-month history of low grade fever, weight loss (5kg), productive cough the first two weeks, epigastric pain and diarrhea. 2-3 loose stools per day for the first 3 weeks.
Epidemiology: Lives in Lima, but born in Tingo María in the high jungle of Peru where he visits at least 4 times per year. Typhoid fever 30 years ago. Physical Examination: T 38.5°C and looking chronically ill. Two painless papular lesions on the face (3-4 mm in diameter) [Image A]. Mouth and oropharynx normal. Generalized non-tender, non-erthematous lymphadenopathy (cervical [Image B], submaxillary, axillary, supraclavicular and inguinal). No rash. Chest clear. Moderate hepatosplenomegaly. Laboratory Examination: Hct. 28%, WBC 6800; 54% polys, 19% lymphs, 16% eos, platelets 761K. Glucose, creatinine and electrolytes normal. LFT normal, total protein 7.1 with albumin of 3.3. Stools for ova and parasites negative. Chest x-ray was normal. Abdominal ultrasound shows diffuse liver and spleen enlargement. HIV ELISA negative but CD4 count is 79. An aspirate and then a biopsy of a cervical lymph node were performed. |
| Diagnosis: Paracoccidioidomycosis, juvenile form. |
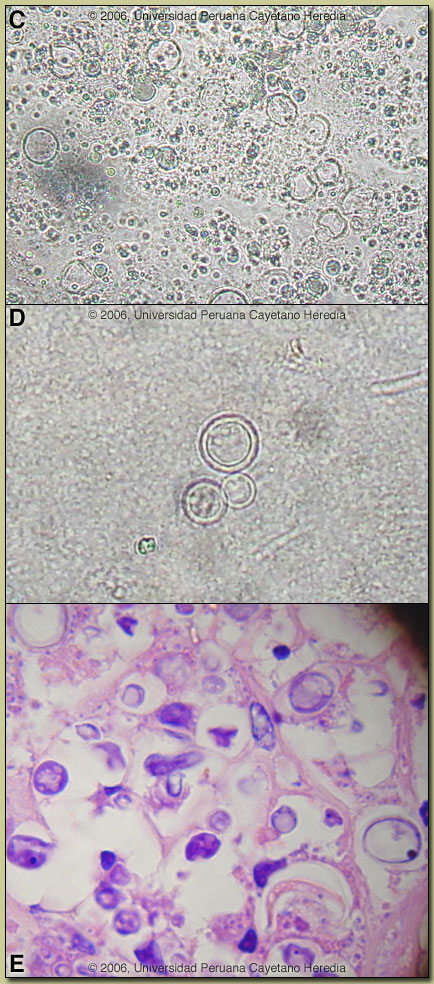 Discussion: Direct KOH preparations of both the lymph node aspirate [Image C] and a sputum sample [Image D] showed spherical cells 10-40 microns in diameter with a thick birefringent cell wall surrounded by several peripheral buds characteristic of Paracoccioides brasiliensis. When completely surrounded by buds a so-called ?pilot-wheel? pattern occurs. Histology of the cervical lymph node disclosed granulomatous lymphadenitis with extensive areas of necrosis and multiple yeast forms characteristic of P. brasiliensis [Image E]. PAS staining also demonstrated yeast forms compatible with paracoccidioidomycosis. Ziehl-Neelsen stain was negative. Direct KOH exam of the skin lesions also showed paracoccidioidomycosis. Direct scrapings or aspirates will be positive in the vast majority of cases of paracoccidioidomycosis with cutaneous lesions. Fungal blood cultures remain negative after 2 weeks; blood cultures would normally be positive in disseminated histoplasmosis. Discussion: Direct KOH preparations of both the lymph node aspirate [Image C] and a sputum sample [Image D] showed spherical cells 10-40 microns in diameter with a thick birefringent cell wall surrounded by several peripheral buds characteristic of Paracoccioides brasiliensis. When completely surrounded by buds a so-called ?pilot-wheel? pattern occurs. Histology of the cervical lymph node disclosed granulomatous lymphadenitis with extensive areas of necrosis and multiple yeast forms characteristic of P. brasiliensis [Image E]. PAS staining also demonstrated yeast forms compatible with paracoccidioidomycosis. Ziehl-Neelsen stain was negative. Direct KOH exam of the skin lesions also showed paracoccidioidomycosis. Direct scrapings or aspirates will be positive in the vast majority of cases of paracoccidioidomycosis with cutaneous lesions. Fungal blood cultures remain negative after 2 weeks; blood cultures would normally be positive in disseminated histoplasmosis.
Paracoccidioidomycosis is most often an indolent and relapsing disease causing chronic pulmonary and mucosal manifestations. The chronic form (adult type) of the disease is believed to represent reactivation of latent infection initially acquired via inhalation. The chronic forms represent approximately 94% of all cases in the experience at our institute (94 patients, up to 2001), and approximately 85% in the Brazilian series [Rev Soc Bras Med Trop. 2003 Jul-Aug;36(4):455-9]. See examples of this in Gorgas Cases 2005-12 and 2004-05]. We have also previously shown a case of the chronic progressive form of the disease [Gorgas Case 2003-07]. This current case is representative of the relatively uncommon “juvenile” acute progressive and disseminated form of the disease which usually (but not always) affects adolescents and young adults – a presentation of paracoccidioidomycosis we have not shown before in the Gorgas Case of the Week series. After an initial self-resolving inhalation event [Clin Infect Dis. 2005 Jan 1;40(1):e1-4], the mononuclear phagocyte system is widely affected with diffuse lymphadenopathy, hepatosplenomegaly, and papular skin lesions with a large burden of yeast forms in all tissues as in our patient. The course is rapidly progressive over weeks in contrast to months or years for the chronic progressive forms. The respiratory system and mucosal surfaces are not involved in the clinical manifestations of the acute juvenile disease but are in the chronic forms. In the present case the CXR is normal and the positive sputum is more likely the result of laryngeal involvement. Differential diagnosis includes histoplasmosis, malignancy, lymphoma, brucellosis, and as a rare manifestation of tuberculosis. Visceral leishmaniasis would be a consideration in endemic areas but this disease does not occur in Peru. Malaria would be a consideration at the stage before appearance of any skin lesions. The juvenile patients manifest with an antigen specific depressed cell mediated immune response to paracoccidiodal antigens in vitro and with negative skin tests. Responsiveness to mitogens and other antigens is normal. The significance of the low CD4 count in this HIV negative patient is a parameter that has not been well studied. In vitro, patients have a predominant Th2 cytokine pattern and eosinophilia, as is the case here. Paracoccidioidomycosis, also known as South American blastomycosis is found in humid forested or lush green areas of the Americas from Southern Mexico south to Uruguay and Argentina. It appears to be most common in Brazil. The exact habitat of the organism is unclear but transmission is described as being entirely by airborne inhalation. However, we have observed cases with only oral lesions apparently associated with the use of tree leaves contaminated with fungal spores as toothpicks. Primary pulmonary infection may be asymptomatic and self-limited but even with treatment will produce at least moderate pulmonary fibrosis. Rural adult males agricultural workers between 30-60 years of age are most affected by the infection. Travelers spending less than 6 months in an endemic area are unlikely to acquire paracoccidioidomycosis. Sulfonamides, ketoconazole, itraconazole, and amphotericin B are all effective therapies. Amphotericin should be reserved for severe cases. Itraconazole 100-200 mg/day for 6-9 months is regarded as the treatment of choice for both the juvenile and chronic forms when it is available and affordable. Relapses are common with less than 6 months therapy and expert opinion is now that 1 year is not necessary. In the developing-world setting, ketoconazole is likely equally effective and is usually less than half the cost. However, 12 months of therapy with ketoconazole is generally recommended. In severe cases with a high yeast burden such as in our case, the practice is to induce such patients with amphotericin B for at least 10 days, then switch to oral itraconazole 200mg per day, to complete a total duration of at least 9 months. Our patient?s fever resolved on Day 6 of therapy and some reduction in lymph node size was noted at that time. |