| 2009 Case #9 |  |
|
|
The Gorgas Course in Clinical Tropical Medicine spent its last week with a 4-day field trip to Iquitos, on the banks of the Amazon River. Iquitos, with a population of approximately 500,000, is the largest city in the world that is reachable only by air and by river. The nearest road ends over 400 km away. The following patient was seen by Gorgas Course participants on the wards of the Military Hospital of Iquitos. |
|
Epidemiology: Military recruit serving at a nearby military base in the jungle. Vaginal intercourse with a regular partner 3 weeks prior to the onset of symptoms. No previous history of sexually transmitted diseases. Physical Examination: [examined and photographed 4 days after therapy initiated]. Afebrile; in no distress. Abnormalities restricted to bilateral inguinal adenopathy. Genital, perianal, rectal examination normal. Laboratory Examination: RPR and ELISA for HIV both non-reactive.
|
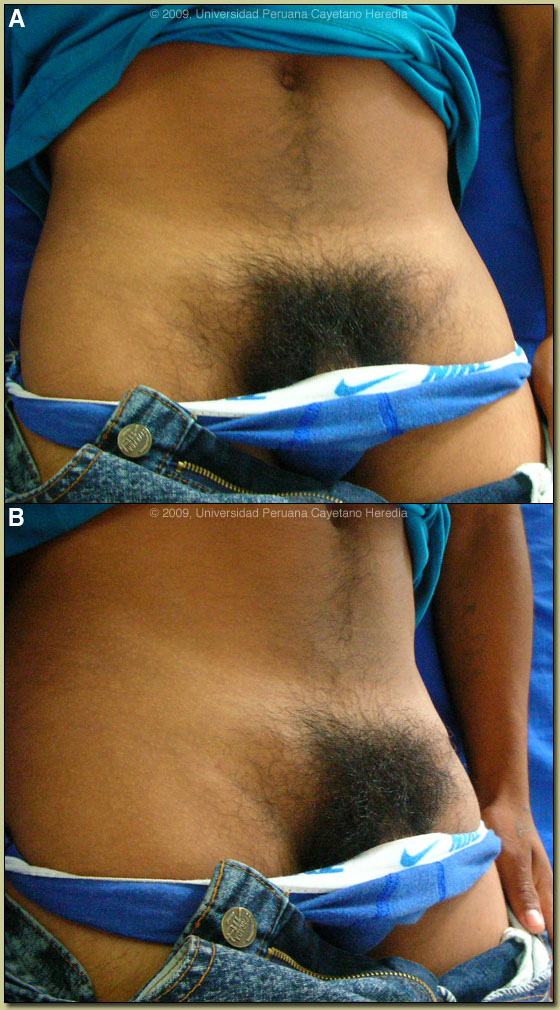
| Diagnosis: Lymphogranuloma venereum (LGV). |
|
Discussion: LGV, which is due to the so-called LGV serovars (L1, L2, L3) of Chlamydia trachomatis, is a sporadic disease in North America and Europe, where it is now very uncommonly seen. In many tropical countries it is still highly endemic, including parts of Africa, India, Southeast Asia, as well as in Amazon regions of Perú and Brasil. In Iquitos, which has a large sex industry due to the simultaneous presence of military bases, oil/gas workers, and narcotics traffickers, infection is highly prevalent and well known to local clinicians. Many recruits consider this activity as a salutary form of mental hygiene to relieve the stress of remote jungle military life. Diagnosis is usually made on clinical grounds as isolation in culture, PCR, LCR, antigen detection, and antibody detection tests are not available. Examination of smears in biopsy material with giemsa staining for inclusion bodies is laborious and of low sensitivity. Ideally, syphilis and HIV serology as well as urethral cultures should be done, but in practice in this highly endemic and resource poor setting rarely are. Even in environments with adequate resources diagnosis is often based on clinical suspicion, epidemiologic information, and the exclusion of other etiologies (of proctocolitis, inguinal lymphadenopathy, or genital or rectal ulcers). Clinically, LGV presents in 3 stages. Primary LGV presents as a small painless papule (or ulcer) at the site of initial infection, which may be penis, labia, vagina, or cervix. It heals spontaneously in a few days and is only noticed by the patient in 3 to 53 percent of cases. Receptive anal intercourse in males or females may result in a primary anal or rectal infection. Similarly, insertive anal intercourse, as is commonly practiced by military recruits visiting sex workers, carries a high acquisition risk. Most often patients present in the secondary stage after the primary lesion has healed and the inguinal lymphadenopathy syndrome is the most common manifestation. However, affected nodes represent a regional lymphadenitis, so peri-rectal and deep iliac nodes may be affected in the case of primary anal, cervical, or posterior urethral infection. There are often constitutional symptoms such as fever, malaise and myalgia. The “inguinal syndrome” is a painful adenopathy developing 2-6 weeks after initial infection and is unilateral in at least two-thirds of cases. Inflammation spreads to overlying skin, which often becomes fixed and matted over underlying lymph nodes. The inguinal ligament separates matted inguinal and femoral lymph nodes forming the pathognomonic “groove sign”. This was not present in this case shown here. Fluctuant buboes may form which may spontaneously rupture or may eventually heal after several months if not treated. Anorectal disease is associated with proctitis, which may be hemorrhagic and with ulceration, which may be mistaken for inflammatory bowel disease. Regional adenopathy in the pelvic, iliac or obturator area may develop and may cause lower abdominal or back pain. LGV is an invasive, systemic infection, and if it is not treated early, LGV proctocolitis might lead to chronic, colorectal fistulas and strictures. Tertiary disease results from lack of treatment, so is uncommonly seen. Chronic lymphatic scarring may result in lymphedema or elephantiasis of the genitalia or breakdown of the overlying skin. Syphilis, chancroid, and herpes may present with inguinal adenopathy but in those cases there is usually a current or recent history of genital ulcer elicited from the patient. Bubo formation does not occur with the latter diseases and if present other diagnostic considerations would be plague, tularemia, or tuberculosis. Treatment continues to consist of doxycycline, or less desirably tetracycline, for 21 days with erythromycin as a second line [Clin Infect Dis. 2007 Apr 1;44 Suppl 3:S147-52]. Azithromycin 1 gm once a week for 3 weeks is likely effective but clinical data is lacking. Buboes may require aspiration through intact skin when they are fluctuant to prevent spontaneous drainage and formation of a chronic fistula: this will also relieve the pain and can be repeated as necessary. Incision or biopsy is contraindicated because of the danger of fistula formation. Individuals with a sexual contact of an LGV case that occurred within 60 days of onset of symptoms should be examined, and if nothing found, treated with doxycycline for 1 week or a single dose of azithromycin |