
|
Gorgas Case 2010-05 |

|
|
This past week, the field trip to Cusco in the Andean highlands took place. Cusco (elevation 3400 m) is the oldest continuously inhabited city in the Americas. This patient was seen on the medical ward of the Social Security Hospital of Cusco. We would like to thank Julieta Tupayachi for bringing this patient from Sicuani, and for helping with the rounds at the Social Security Hospital in Cuzco.
History: 43 year-old male first presented with a 2-year history of progressive dyspnea and dry cough. Two months later an acute deterioration occurred when he noticed that the cough became more severe with production of large amounts of liquid sour tasting salty sputum that did not appear purulent. The patient could not afford detailed medical evaluation. The dyspnea improved after this episode but has subsequently worsened. There have been some episodes of fever to which he received oral antibiotics of an unknown nature. Epidemiology: Born in the highlands of Perú where he worked raisingcattle. The patient has also worked in illegal gold-mining operations inthe Peruvian jungles for 25 years. No known TB contacts. No HIV riskfactors. Physical Examination: Afebrile, tachypnea (30 respirations per minute),pulse 90 per minute. Multiple inactive scars on skin from earlier episodesof leishmaniasis. Normal oral mucosa. Marked reduction in breathsounds in the right hemithorax with dullness; inspiratory rales in the base ofthe left lung. Rest of the exam is normal. Laboratory Results: Hemoglobin 14.2; WBC 7400 with normal differential,no eosinophils. Chest x-rays: Image A was taken at theinitial presentation; Images B and C were taken 2 months laterat the time of the acute deterioration. CT scan of the chest [ImageD] was taken 8 months later at the time of examination by the Gorgasparticipants. Abdominal ultrasound: normal. 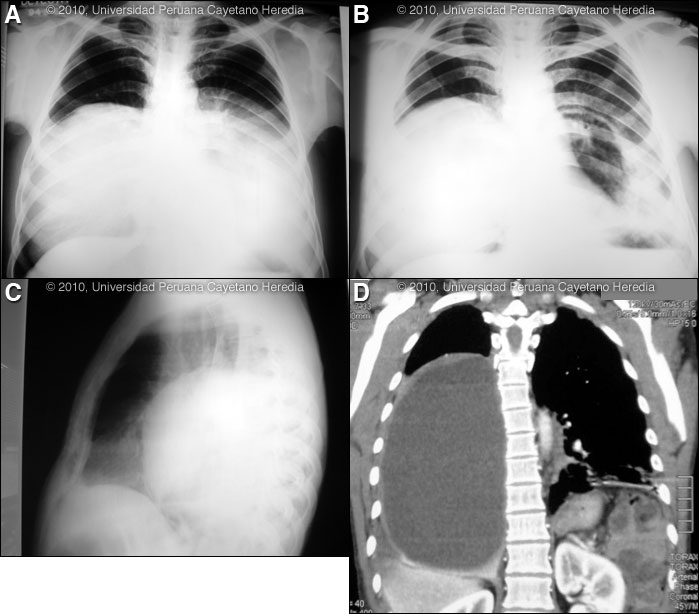

|
|
Diagnosis: Echinococcus granulosus. Bilateral pulmonary hydatid cysts. Acute rupture of left cyst into a main bronchus.
Discussion: A Western blot taken before the acute rupture was strongly positive for E. granulosus. The expectoration of large amounts of salty fluid is highly characteristic of this catastrophic event. The CT scan showed a giant cystic lesion that occupies ¾ of the right hemithorax with displacement of the mediastinum. The residual cavity in the posterior left lung has surrounding parenchymal inflammatory infiltrates. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. This patient had ongoing exposure to dogs while working in the cattle raising industry. Sheep are the normal intermediate hosts. Larval cysts expand slowly over years or decades, becoming symptomatic as they impinge on other structures by virtue of their size. Spontaneous cyst rupture as occurred here happens in the minority of cases but is not rare. The cysts contain hundreds of viable protoscoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new protoscoleces on an ongoing basis. Each protoscolex is capable of becoming a new daughter cyst should the original cyst rupture or be ruptured. However it is unusual to see secondary pulmonary cysts from bronchial seeding after a rupture of a cyst into a bronchus, as in this case. This is probably due to adhesion of protoscoleces to mucus secretions in the airways and to ciliary movement that will eliminate the protoscoleces subsequent to the cough reflex. An example of seeding of the pleural cavity after an intraparenchymal rupture is seen in a previous case of the week [see Gorgas Case 2005-10]. Cystic hydatid disease due to E. granulosis is common in sheep and cattle raising areas worldwide. Most primary infections involve a single cyst. 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 18% will also have a hepatic cyst. Bilateral lung hydatid cysts are present in 6% of adults but in up to 30% of children in whom pulmonary involvement is generally more frequent [Pediatr Radiol. 1978 Sep 26;7(3):164-71]. In our experience in Perú 3.8% of pulmonary cysts are bilateral. Pulmonary hydatid disease affects the right lung in 60% of cases. Serology is usually positive with hepatic cysts but sensitivity drops below 50% with solitary pulmonary cysts even when the cyst is large. With the large burden of disease in this patient’s lung a positive serology would be expected. Praziquantel is the most potent scolicidal drug and is the drug of choice for all adult tapeworms. However, praziquantel cannot penetrate the hydatid cyst wall, so it is only useful as an acute therapy when a cyst ruptures (spontaneously or due to surgical mishap) and scoleces are lying free before encysting again. Albendazole is the therapy of choice for intact cysts that are not operable, such as when there are multiple or disseminated cysts. A trial of albendazole may also be considered for solitary cysts that are less than about 10 cm. Response is generally slow and only complete in a minority of cases. Surgical resection is the therapy of choice for large intact cysts. Experimental protocols using combined praziquantel and albendazole are underway in several places, but a patient with extensive disease would still not be a candidate for medical therapy only. The patient is going to be transferred to Lima for further surgical management of his disease. The surgical approach to bilateral hydatid disease of the lungs has not been the subject of any systematic trials or retrospective reviews of outcomes and the approach is surgeon dependent. Bilateral disease may be managed by one- or two-stage surgery. Some prefer two-stage thoracotomy, operating on the side with the larger, ruptured, or infected cyst first as a more cautious approach. However, when feasible, many consider a median sternotomy single-stage combined resection to be the approach of choice, and it is less traumatic and painful for the patient. Visualization of a typical pulmonary hydatid cyst at the time of surgery was shown in one of our previous cases [see Gorgas Case 2008-02]. Technical aspects of surgery are reviewed [Respiration. 2000;67(5):539-42; Eur Respir J. 2003 Jun;21(6):1069-77]. In the case of pulmonary cysts many surgeons feel that cyst softening that may occur with perioperative albendazole makes the operative procedure more complicated and increases the risk of rupture at the time of resection. No data from trials is available.
|