 |
Gorgas Case 2011-05 |
 |
|
This past week, the field trip to Cusco in the Andean highlands took place. Cusco (elevation 3400 m) is the oldest continuously inhabited city in the Americas. This patient was seen on the inpatient department of the Regional Hospital of Cusco.
History: Previously healthy, 3-year-old girl admitted with one-year history of epigastric pain, 3kg weight loss in the 3 months prior to admission, and fever, cough and respiratory distress one month before admission. She was diagnosed with pneumonia and treated with antibiotics at a local health centre with no improvement. Epidemiology: Born and lives in a rural agricultural town in the highlands of Cuzco Department; received complete immunizations; previously healthy. Patient helps in tending sheep, cattle, and other farm animals. No specific TB exposures. Physical Examination: Respiratory rate: 60, HR: 130, Temperature: 38.5°C. Acutely ill with moderate respiratory distress. No edema, no cyanosis, HEENT: normal. Lungs: intercostal retractions on normal respiration with no rales. Enlarged liver (4 cm below right margin). No splenomegaly or lymphadenopathy. Chest x-ray and CT scan are shown [Images A-E]. Laboratory: Hct 41. WBC 10,600 (3 band, 52 neutrophils, 6 Eosinophils, 4 monos, 35 lymps). Glucose 101, BUN 17. Creatinine normal. 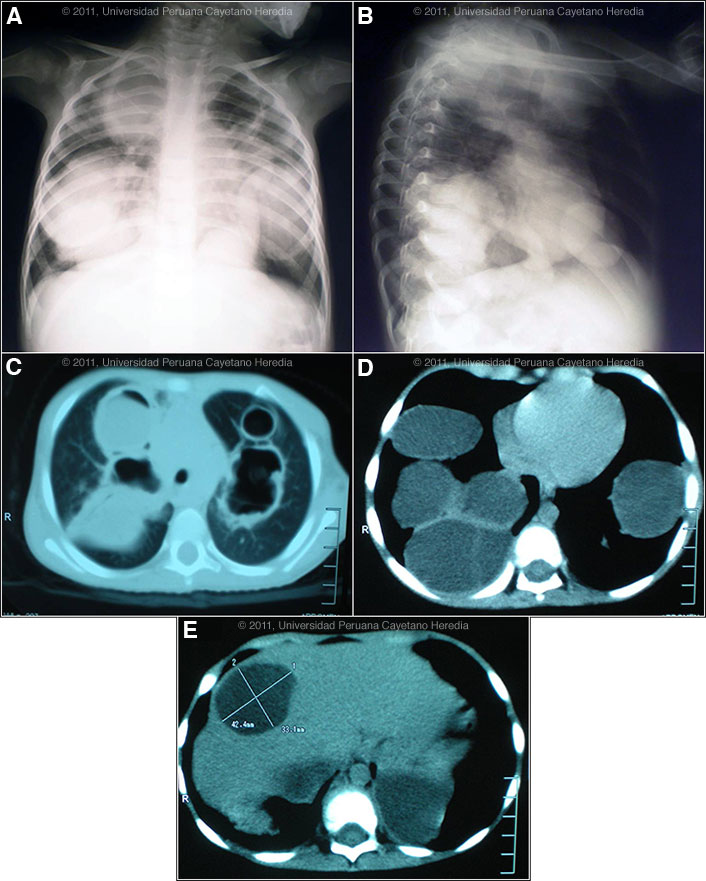
 |
|
Diagnosis: Pulmonary and hepatic hydatid cysts due to Echinococcus granulosus.
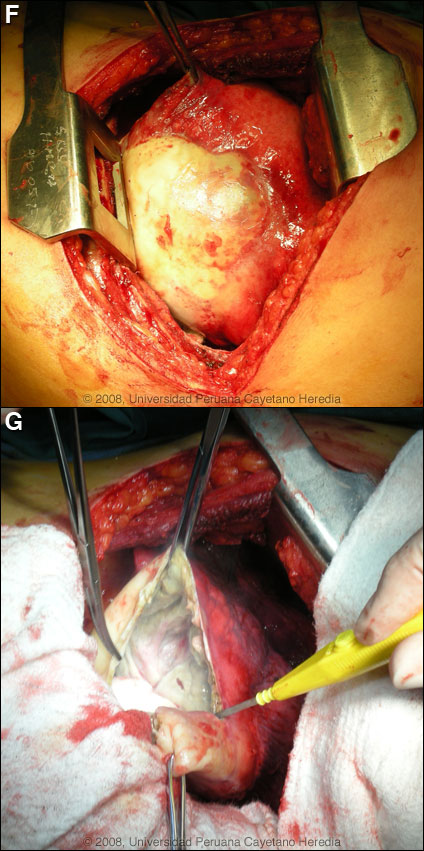
Discussion: The large cysts on chest x-ray and CT scan are diagnostic of hydatid disease. See previous cases of the week for radiologic presentations in those cases [Gorgas Cases 2010-05, 2008-02, 2001-01, 2005-10]. In this case, the density of the cyst fluid in the chest lesions, some perilesional infiltrate and the fever are highly suggestive of bacterial superinfection of the cysts. This may occur due to a small spontaneous tear in a cyst or via a bronchial fistula (possible fistula here but not clear from the images). In adults the expectoration of salty-tasting fluid is highly characteristic of a fistula or frank rupture of a cyst into a bronchus, but children may not be able to describe this. Western blot for E. granulosus was pending at the time of our visit. Images F & G show a pulmonary hydatid in situ in another patient of ours [Gorgas Case 2008-02]. Serology is usually positive with hepatic cysts but sensitivity drops below 50% with solitary pulmonary cysts even when the cyst is large. With the large burden of disease in this patient’s lung and liver a positive serology would be expected. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. This patient had ongoing exposure to dogs while her parents were working raising cattle and sheep. Sheep are the normal intermediate hosts. In general, disease is diagnosed in adulthood as larval cysts expand slowly over years or decades, becoming symptomatic as they impinge on other structures by virtue of their size. The cysts contain hundreds of viable protoscoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new protoscoleces on an ongoing basis. Each protoscolex is capable of becoming a new daughter cyst should the original cyst rupture or be ruptured. However it is unusual to see secondary pulmonary cysts from bronchial seeding after a rupture of a cyst into a bronchus, as may have occurred in this case. This is probably due to adhesion of protoscoleces to mucus secretions in the airways and to ciliary movement that will eliminate the protoscoleces subsequent to the cough reflex. Cystic hydatid disease due to E. granulosis is common in sheep and cattle raising areas worldwide. Most primary infections involve a single cyst. In adults, 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 18% will also have a hepatic cyst. Bilateral lung hydatid cysts are present in 6% of adults but in up to 30% of children [Pediatr Radiol. 1978 Sep 26;7(3):164-71]. In our experience in Perú 3.8% of pulmonary cysts are bilateral. A number of series from Europe consider pulmonary involvement to be more common than hepatic in children but a recent series from Latin America found the opposite [Rev Argent Microbiol. 2009 Apr-Jun;41(2):105-11]. In that series, 59% of pediatric cases were male, 28% of pediatric cases were under age 6, and average cyst size was only 2.6 cm. Thus, the extensive disease in this child age 3 is unusual and one can hypothesize infection at a very young age with either (1) a very large inoculum seeding widely, or (2) a subsequent traumatic rupture into a bronchus with wide seeding. Many experienced pediatric clinicians have observed faster than usual growth of lung cysts in young children due to laxer and more permissive parenchymal tissue when compared to adults. The presentation of pulmonary hydatid varies widely, making a uniform treatment recommendation impossible. For single, intact, uncomplicated pulmonary cysts surgery is the treatment of choice, though a trial of albendazole alone may used alone on small (<5 cm), uncomplicated lung cysts. In term of possible drug therapy, praziquantel is the most potent scolicidal drug and is the drug of choice for all adult tapeworms. In hydatid disease, praziquantel is unlike albendazole and does not penetrate the cyst wall or produce measurable concentrations in cyst fluid. Praziquantel is also ineffective against the germinal membrane of cysts, but is able to reliably and quickly kill free protoscoleces [Acta Trop. 2009 Aug;111(2):95-101]. Thus, praziquantel is useful as an acute therapy when a cyst ruptures (spontaneously, or intra-operatively due to surgical mishap) and scoleces are lying free before encysting again. A recent international consensus document [Acta Trop. 2010 Apr;114(1):1-16] recommends routine pre-operative praziquantel/albendazole therapy for liver cysts only but specifically recommends that albendazole should be avoided pre-operatively in larger lung cysts as softening may complicate surgery. There is no data or experience with the theoretically enticing concept of pre-operative praziquantel for lung lesions. In Perú, albendazole is the therapy of choice for intact cysts that are not operable, such as when there are multiple or disseminated cysts. A trial of continuous albendazole may also be considered for solitary cysts that are less than about 5 cm. Response is generally slow. Combined praziquantel and albendazole for medical therapy of liver or lung hydatid has been reported in several small uncontrolled series and experimental protocols examining combination therapy using are underway in several places. Transfer to Lima for further management of her disease was advised but the patient declined. She is being treated with ceftriaxone and clindamycin for the superinfection and we have recommended she receive several months of albendazole to see if there is any response as surgery would be difficult in a complicated case like this with multiple cysts. Ideally, however, the patient should be treated medically on a specialized unit in case of a catastrophic cyst rupture, which would then require urgent surgery. Any surgical intervention at any point should preserve as much lung parenchyma as possible even at the expense of leaving some intact cysts. In the event of general clinical deterioration, radical procedures are often required for extended parenchymal involvement, severe pulmonary suppuration, and complications.
|