 |
Gorgas Case 2012-05 |
 |
|
This past week, the field trip to Cusco in the Andean highlands took place. Cusco (elevation 3400 m) is the oldest continuously inhabited city in the Americas. The following patient was seen in the inpatient department of the 200-bed Cusco Regional Hospital.
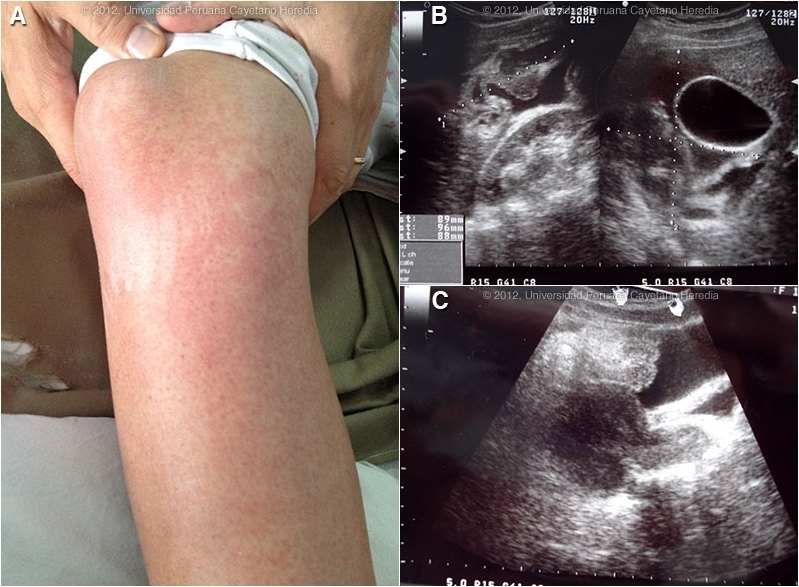  History: 17-year-old female sustained a traumatic kick to the right thorax while playing with a child. Soon thereafter she developed localized RUQ pain that after 12 hours became severe generalized abdominal pain for which she was given naproxen. 12-18 hours later she developed a generalized urticarial rash preceding her presentation the emergency department with worsening abdominal pain. No fever, no respiratory symptoms, no diarrhea, no jaundice. Epidemiology: Resident of Cusco city but spent her early childhood in the highlands with exposure to farm animals. No known TB exposure, no sex partners, no drug use. Up to date on vaccines. Physical Examination: Afebrile. Normotensive. Chest clear. Abdomen: diffusely tender with normal bowel sounds, no peritoneal signs, no hepatosplenomegaly. Skin: diffuse intensely pruritic rash with excoriation [Image A]. Laboratory Results: Hemoglobin 11.9, WBC 5.5 with 70 neutrophils, 9 monos, 18 lymphs, 3 eosinophils. Normal electrolytes, renal function, and liver function. CXR normal. Abdominal ultrasound is shown [Images B, C].
|
|
Diagnosis: Echinococcus granulosus. Acute traumatic rupture of hydatid cyst.
 Discussion: The ultrasound showed a 10 X 9 X 9 cm homogeneous fluid filled cyst (stage CE 3a) with detached endocyst membranes (originally forming the cyst wall) floating in the cyst cavity. Free peritoneal fluid was present. Based on the ultrasound the patient was taken to emergency laparotomy where a ruptured cyst with hydatid fluid throughout the peritoneal cavity was found. Total cystectomy with copious lavage of the peritoneal cavity was carried out. Image D shows a gross surgical specimen from a similar case from our files. Previous hepatic hydatid cases we have shown are Gorgas Cases 2003-03 and 2011-05. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. This patient had ongoing exposure to dogs while growing up. Sheep are the normal intermediate hosts. In general, disease is diagnosed in adulthood as larval cysts expand slowly over years or decades, becoming symptomatic as they impinge on other structures by virtue of their size. The cysts contain hundreds of viable protoscoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new protoscoleces on an ongoing basis. Each one of these hundreds of protoscoleces is capable of becoming a new daughter cyst in the peritoneal or thoracic cavity should the original hepatic or pulmonary cyst rupture or be ruptured. Cystic hydatid disease due to E. granulosus is common in sheep and cattle raising areas worldwide. Most primary infections involve a single cyst. In adults, 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 18% will also have a hepatic cyst. Albendazole is the therapy of choice for intact cysts that are not operable, such as when there are multiple or disseminated cysts. A trial of continuous albendazole may also be considered for solitary cysts that are less than about 5 cm. Response is generally slow. Albendazole should be immediately instituted in ruptures whether they be spontaneous, post-traumatic or the result of a surgical accident. Praziquantel is the most potent scolicidal drug and is the drug of choice for all adult tapeworms. In hydatid disease, praziquantel is unlike albendazole and does not penetrate the cyst wall or produce measurable concentrations in cyst fluid. Praziquantel is also ineffective against the germinal membrane of cysts, but is able to reliably and quickly kill free protoscoleces [Acta Trop. 2009 Aug;111(2):95-101.]. Thus, praziquantel is useful as an acute therapy when a cyst ruptures (spontaneously, or intra-operatively due to surgical mishap) and scoleces are lying free before encysting again. A recent international consensus document [Acta Trop. 2010 Apr;114(1):1-16.] also recommends routine pre-operative praziquantel/albendazole therapy for liver cysts in case of surgical spillage. Combined praziquantel and albendazole for medical therapy of liver or lung hydatid has been reported in several small uncontrolled series and experimental protocols examining combination therapy using are underway in several places. Our patient had urticaria and pruritus that persisted for over 5 days despite aggressive anti-histamine treatment. The timing, mechanisms and pathogenesis of anaphylactic reactions in cystic echinococcosis is not understood but explained by most as the disruption of the integrity of the cyst wall with spillage of allergenic cyst contents into the patient’s circulation. Despite 75% of infected patients having specific IgE antibodies, rupture of echinococcal cysts does not always or even commonly lead to anaphylactic reactions. Two case series have looked at anaphylaxis after either cyst spillage secondary to percutaneous procedures or after intra-operative rupture and in each case the reaction was reported to have been almost immediate [Am J Trop Med Hyg. 2011 Sep;85(3):452-5., PLoS Negl Trop Dis. 2011 Jun;5(6): e1154.]. Our patient did not develop urticaria for about 30 hours after the trauma and did receive a few doses of naproxen. However, the latter does not explain the prolonged refractory symptoms and it is possible that the trauma did not lead to immediae spillage of cyst contents. Eosinophilia is common in this situation and the CBC has been repeated twice more during the hospitalization with similar results. The patient has begun albendazole therapy with plans for a prolonged course. Praziquantel will be started once it can be procured, as it is not normally available in Cusco. Acknowledgements: We thank Dr. Miguel Cabada, Gorgas Course Clinical Coordinator in Cusco and Professor Enrico Brunetti, University of Pavia for helpful discussions.
|