 |
Gorgas Case 2013-01 |
 |
|
The Gorgas Courses in Clinical Tropical Medicine are given at the Tropical Medicine Institute at Cayetano Heredia University in Lima, Perú. For the 13th consecutive year, we are pleased to share interesting cases seen by the participants that week during the February/March course offerings. Presently the 9-week Gorgas Course in Clinical Tropical Medicine is in session. New cases will be posted every Tuesday/Wednesday for the next nine weeks. Each case includes a brief history and pertinent digital images, followed by a link to the actual diagnosis and a brief discussion.
David O. Freedman & Eduardo Gotuzzo
Course Directors |
|
The following patient was seen on the Surgical Ward of the 450-bed Cayetano Heredia National Hospital.
 History: 17 yo previously healthy male presenting with a 6-month history of cough, expectoration of whitish sputum, frequently with blood streaking, and left pleuritic chest pain. Subjective feeling of fever, but no night sweats. A left thoracentesis yield fluid but no acid fast organisms and 3 sputum was negative for AFB. He was diagnosed with tuberculosis but had no response to therapy and was referred to us.
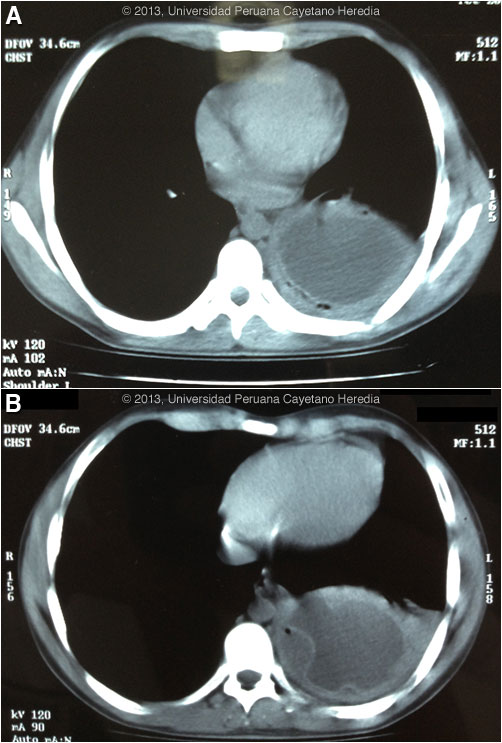
Epidemiology: Born and lives in Huánuco in the highlands where he works in construction. Grew up on a farm with various animals including dogs, sheep, cows, and pigs. No travel. No known TB exposure. No ill contacts. Physical Examination: Afebrile. Normal examination except for decreased breath sounds and dullness in the left base. Laboratory Results: Hb 14.0, WBC 17,000 with 77 PMNs, no monocytes, no eosinophils. Normal renal and hepatic function. HIV negative. Chest CT scan is shown in Images A & B.
|
|
Diagnosis: Echinococcus granulosus.
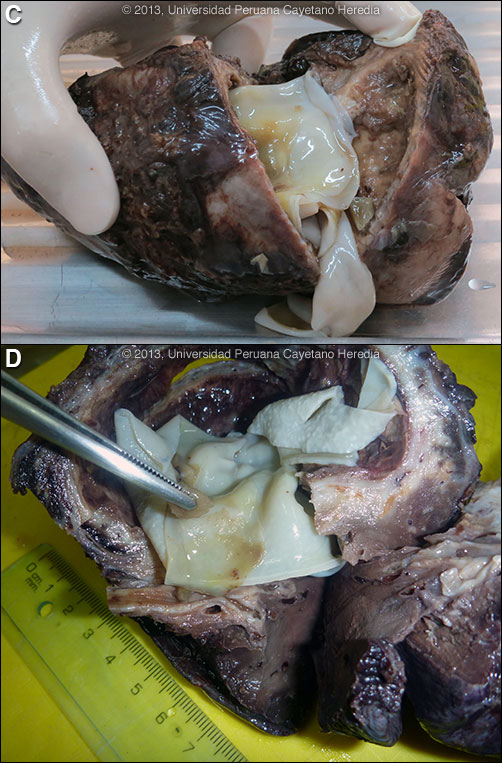
Discussion: The fluid-filled pulmonary cyst on CT scan with detached membrane [Image B] is diagnostic of hydatid disease without any further serology (usually a western blot) or diagnostic procedure. The air between the detached parasite membrane and the cavity wall is indicative of erosion into a bronchus. Serology is usually positive with solitary hepatic cysts but sensitivity drops below 50% with solitary pulmonary cysts even when the cyst is large such as this. Treatment of pulmonary hydatid is surgical and most surgeons will not operate if pre-operative albendazole has been given as this softens the cyst wall somewhat. The patient underwent a left hemi-lobectomy. Image C shows the resected lung with the large cavity lined by the hydatid membanes. Image D shows the acellular lamellated white parasite membrane stripped away from the cyst cavity. The forceps are holding the inner germinal membrane of the cyst, which is the layer that is alive and contains the cells that continuously produce new tapeworm scoleces. Previous pulmonary hydatid cases we have shown are Gorgas Cases 2005-10 and 2011-05. In adults the expectoration of salty-tasting fluid with or without pieces of white membranous material is highly characteristic of a fistula or frank rupture of a cyst into a bronchus, but this patient did not describe this. Sputum production and fever may have been due to a small fistula with resulting bacterial superinfection. He was treated with ceftriaxone on admission. Human hydatid disease secondary to Echinococcus granulosus is caused by the larval form of this dog tapeworm. Humans ingest the tapeworm eggs in environments contaminated by canine feces and become accidental intermediate hosts. This patient had ongoing exposure to dogs during his whole life. Sheep are the normal intermediate hosts. In general, disease is diagnosed in adulthood as larval cysts expand slowly over years or decades, becoming symptomatic as they impinge on other structures by virtue of their size. The cysts contain hundreds of viable protoscoleces capable of becoming adult tapeworms upon ingestion by a definitive host such as the dog. The internal germinal membrane lining the cyst produces new protoscoleces on an ongoing basis. Each protoscolex is capable of becoming a new daughter cyst should the original cyst rupture or be ruptured. Cystic hydatid disease due to E. granulosis is common in sheep and cattle raising areas worldwide. Most primary infections involve a single cyst. In adults, 65% of solitary cysts are found in liver, 25% in lung and the rest in a wide variety of other organs including kidney, spleen, heart, bone and brain. In patients with a pulmonary cyst, approximately 18% will also have a hepatic cyst. The patient has not pursued abdominal imaging at this point. Surgery may involve excision of the cyst or resection of the cyst and the immediate surrounding parenchyma. Despite the lack of consensus, the currently most accepted surgical treatment for lung hydatic is complete excision using parenchyma-preserving methods, such as cystostomy, intact cyst enucleation or removal after needle aspiration preserving as much lung parenchyma as possible. Resection techniques such as pneumonectomy, segmentectomy should be reserved to cysts involving whole hemithorax or the whole segment respectively; and lobectomy generally should be performed only in large abscessed cysts. Most surgeons use pads soaked in hypertonic saline to protect the operatory field from spillage and subsequent seeding of new cysts. Albendazole is the therapy of choice for intact cysts that are not operable, such as when there are multiple or disseminated cysts. A trial of continuous albendazole may also be considered for solitary cysts that are less than about 5 cm. Response is generally slow. Albendazole should be immediately instituted in ruptures whether they be spontaneous, post-traumatic or the result of a surgical accident. Praziquantel is the most potent scolicidal drug and is the drug of choice for all adult tapeworms. In hydatid disease, praziquantel is unlike albendazole and does not penetrate the cyst wall or produce measurable concentrations in cyst fluid. Praziquantel is also ineffective against the germinal membrane of cysts, but is able to reliably and quickly kill free protoscoleces [Acta Trop. 2009 Aug;111(2):95-101]. Thus, praziquantel is useful as an acute therapy when a cyst ruptures (spontaneously, or intra-operatively due to surgical mishap) and scoleces are lying free before encysting again. A recent international consensus document [Acta Trop. 2010 Apr;114(1):1-16] also recommends routine pre-operative praziquantel/albendazole therapy for liver cysts in case of surgical spillage. Combined praziquantel and albendazole for medical therapy of liver or lung hydatid has been reported in several small uncontrolled series and experimental protocols examining combination therapy using are underway in several places.
|