By Ranjit Kaur, OD, 2020 Family Practice Resident
The pandemic took a hard grip on the healthcare system, including Optometry. The last few months introduced us to challenges we were not quite prepared for as a healthcare system, and Doctors of Optometry have stood strong in response to the COVID-19 crisis. We focused on providing urgent and emergent care to our patients to reduce the burden on emergency departments, incorporating telemedicine into the practice in order to reduce exposure risk to the more vulnerable patients, and adopting a virtual clinical education platform for our students learning from home.
After graduating from Western University of Health Sciences College of Optometry, I decided to pursue a residency in family practice with an emphasis on ocular disease at the University of Alabama at Birmingham School of Optometry. Although I was skeptical at first to move across the country, it turned out to be the best decision I could have made. From confidence in independent patient care, management of anterior and posterior segment diseases, giving COPE approved lectures, teaching optometry students, and developing interprofessional skills, it clearly could not get any better than this. Until the introduction of COVID-19, that is.
Beginning early March, all clinical operations at UAB Eye Care (UABEC) were temporarily suspended to ensure the safety of our patients, staff, students, and faculty. It was not practical to completely close its doors; UABEC serves nearly 200 patients daily during normal operations. emergent and urgent cases for existing and new patients needing immediate access to eye care. Although I was familiar with the on-call protocol as it is included in the UABSO Residency curriculum, there was an increase in the volume and severity of cases during this uncertain time, which certainly contributed to massive growth in the learning curve. To limit exposure, I was the only resident, along with one other faculty member, to provide direct patient care in clinic. With the help of my co-residents and faculty, I was able to gain clinical knowledge and skills in a short period of time. I had the opportunity to diagnose, treat, and manage some of the most critical ocular conditions: multiple foreign body removals in pediatrics and adults, corneal abrasions, chronic uveitis, corneal ulcers, sudden loss of vision. As a 2020 graduating resident, I am proud to have been part of a university that provides opportunities to advance clinical knowledge while supporting collaborative and independent learning. I will now highlight some cases that required rigorous and timely treatment during the pandemic.
 Figure 1: PROKERA® placed on the right eyeA 54-year-old Caucasian male, who had been working near his swimming pool that contained a sodium hypochlorite chemical agent, presents with pain (10/10), light sensitivity (8/10), and periorbital edema in both eyes for one day now, progressively worsening through the day. His entering visual acuity is 20/100 in the right eye and 20/60 in the left eye, no improvement with pinhole. Upon clinical examination, his signs and symptoms were evident for a corneal melt of the right eye and corneal toxicity in both eyes secondary to sodium hypochlorite as the inciting agent. After thorough irrigation of both eyes, I performed corneal debridement followed with insertion of a PROKERA® amniotic membrane on the right eye (Figure 1) and a bandage contact lens on the left eye. With proper therapeutic drops and a series of follow-ups, his vision slowly reversed back to 20/20.
Figure 1: PROKERA® placed on the right eyeA 54-year-old Caucasian male, who had been working near his swimming pool that contained a sodium hypochlorite chemical agent, presents with pain (10/10), light sensitivity (8/10), and periorbital edema in both eyes for one day now, progressively worsening through the day. His entering visual acuity is 20/100 in the right eye and 20/60 in the left eye, no improvement with pinhole. Upon clinical examination, his signs and symptoms were evident for a corneal melt of the right eye and corneal toxicity in both eyes secondary to sodium hypochlorite as the inciting agent. After thorough irrigation of both eyes, I performed corneal debridement followed with insertion of a PROKERA® amniotic membrane on the right eye (Figure 1) and a bandage contact lens on the left eye. With proper therapeutic drops and a series of follow-ups, his vision slowly reversed back to 20/20.
An 18-year-old African American male reports waking up with a constant red filter in front of the left eye. His medical and ocular history are unremarkable with no reports of trauma. The patient is also not currently taking any medications. Vision in the right eye is 20/20 and 20/50 in the left eye, no improvement with pinhole. Preliminary testing and anterior segment findings are within normal limits. Dilated fundus examination revealed boat-shaped macular pre-retinal hemorrhage in the left eye and moderate amount of retinal hemorrhages and Roth spots in both eyes (Figure 2). A complete hematological profile was ordered after discussing differentials with the patient’s primary care physician. With a white blood cell count of 331,000 per microliter of blood, the diagnoses of chronic myeloid leukemia (CML) was established and the patient was immediately admitted into the hospital to begin treatment. A combination of tyrosine kinase inhibitors (TKIs), dasatinib 100 mg, and an antineoplastic agent, hydroxyurea 1000 mg, was initiated. Since starting the therapy, his white blood cell count reduced from 331,000 to 5,250 per microliter of blood. The therapeutic drug response and efficacy are closely monitored by his oncologist. Because these ocular findings reflect the severity of the disease process, a prompt referral and immediate treatment are warranted to improve the patients’ quality of life and life expectancy.
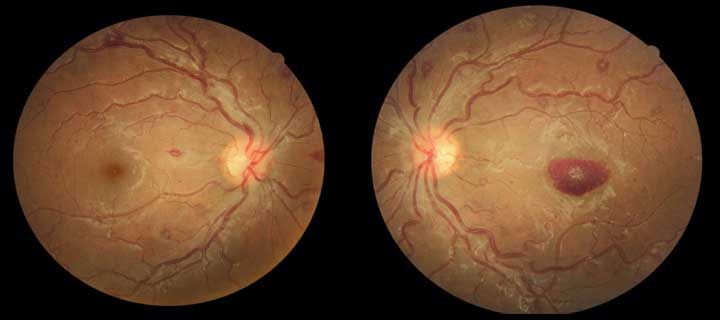 Figure 2: Multiple Roth spots, both eyes and Pre-retinal hemorrhage left eye
Figure 2: Multiple Roth spots, both eyes and Pre-retinal hemorrhage left eye
A 51-year-old Caucasian male presents with sudden peripheral vision loss in both eyes, first noticed 3 weeks ago. This vision loss prompted him to schedule a visit with his local optometrist, who claimed it to be part of an aging process and prescribed progressive lenses. After multiple episodes of blurred vision and peripheral loss, he called UABEC for a second opinion. After a thorough history and clinical findings, including gait, cranial nerve testing, tangent screen, and Humphry visual field (Figure 3), an immediate stroke workup was ordered. As a result, the patient was diagnosed with three brain hemorrhages which led to a permanent visual field loss that may have been avoided if the local optometrist had made a prompt referral.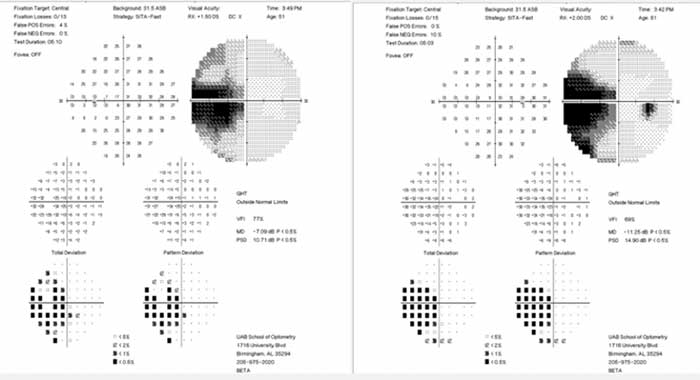 Figure 3: HVF 30-2: left incomplete homonymous hemianopsia
Figure 3: HVF 30-2: left incomplete homonymous hemianopsia
A 39-year-old Caucasian male calls complaining of eye pain, constant mucopurulent discharge, significant blur, redness, and swollen eyes, progressively worsening for 3 days. He reports no improvement with Zyrtec and allergy drops. His entering visual acuity was 20/30+ in both eyes, 3+ diffuse injection with chemosis of bulbar conjunctiva, inflammation of palpebral conjunctiva, and subepithelial infiltrates in both corneas. Due to the mixed etiology of bacterial and viral conjunctivitides, he was treated in-office with 5% betadine eye wash. After just one day of treatment, he reported improvement in eye pain, discharge, redness, and lid swelling (Figure 4).
 Figure 4: Initial presentation (left) and 1 day post Betadine eye wash (right)
Figure 4: Initial presentation (left) and 1 day post Betadine eye wash (right)
After graduating from optometry school, my goal was to complete a residency in family practice to enhance my clinical and professional education. This additional year of training has given me so much more. As an optometry resident, I was able to impact the lives of multiple patients. Personalized thank you cards, flowers, texts, and calls were some of the ways they showed gratitude to me for providing optimal care during this time of uncertainty (Figure 5). Health care workers on the front lines across the nation were expected to provide excellent care during the COVID-19 pandemic. As optometrists, we should not forget that we are the primary care doctors in eye care. It is our duty to diagnose ocular conditions and make appropriate referrals, when necessary. As a Class of 2020 graduating Resident, I am confident to saying that I am leaving my UAB family with unconventional skills and abilities that can benefit patient care in more ways than ever before.
 Figure 5: Thank you card from patient seen during the pandemic
Figure 5: Thank you card from patient seen during the pandemic