 |
2013 Case #4 |  |
| The following patient was seen in the outpatient department of the 36-bed Tropical Disease Unit at Cayetano Heredia National Hospital. |
|
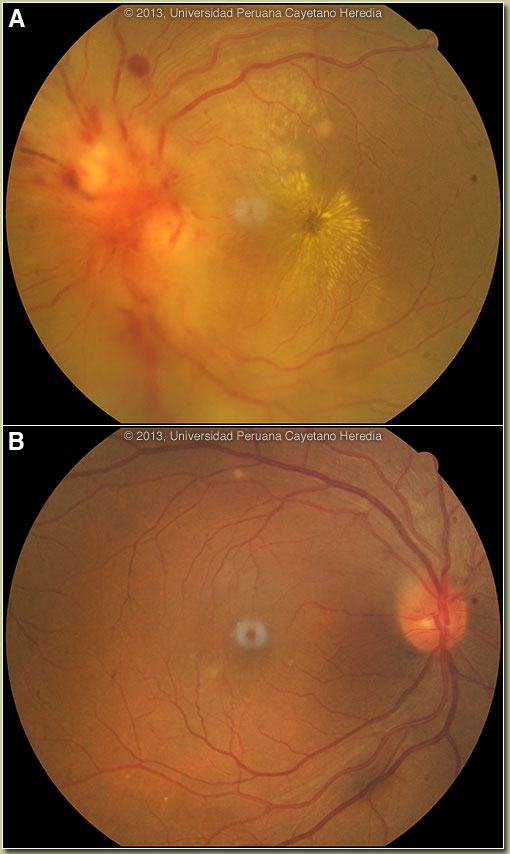
Epidemiology: Born and lives in Lima with no history of travel. Married, monogamous, middle-class, with one child and two cats. Does not work outside the home. No history of illicit drug use, sexually transmitted disease or known TB contact. Regular Limeña dietary habits including ceviche, cheese from the market, and fruits and vegetables from all over the country. Physical Examination: Afebrile, normal vital signs. Chest clear. Cardiac exam without rubs, murmurs or extra sounds. No hepatosplenomegaly; no lymphadenopathy. No skin lesions found. Visual acuity right eye 20/20; left eye finger counting only. Image A shows the left retina with a severely obliterated and swollen optic nerve head. Hemorrhage is centered on the nerve head and is from within the nerve head, not scattered in the retina. Observed is an obvious “stellate maculopathy”, the star shaped pattern of lipid that collects around the fovea when WBCs and exudative inflammatory material is pushed from the optic nerve border and spills over into the macular zone. Right eye is normal [Image B]. Laboratory Results: Hematocrit 42. Normal WBC with normal differential. Normal hepatic and renal function. Normal serum glucose. HIV, ANA, and ANCA negative.
|
| Diagnosis: Cat-scratch disease (CSD) with neuroretinitis due to Bartonella henselae. |
|
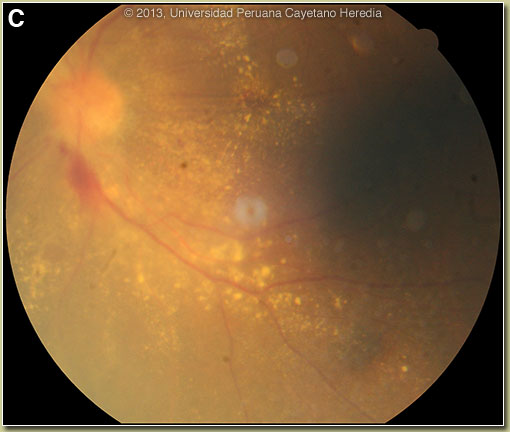
On further questioning the patient recalled that a neighbor’s cat had jumped on her face several weeks earlier, leaving just a short-lived scratch but no other local lesion or regional adenopathy (called Parinaud’s syndrome when it occurs). Neuroretinitis, of which this is a severe example, is a severe optic neuritis with secondary retinal involvement. The retina just beyond the macula in this case is normal. There is no diffuse choroidits or retinitis or vasculitis. There is no retinal vascular disease (an angiogram, not shown, was normal). No flame heme or peripheral heme is seen. The most common cause of this picture in a developed country like the USA is cat-scratch disease (CSD). Brucellosis, a common disease in Perú would generally have more of a uveitis, hazy vitreous component or anterior uveitis, and less severe disk changes, but is still very possible in this patient. Stellate maculopathy with the neuroretinitis can be seen in the entities discussed in the above section. Syphillis usually has more chorioretinitis and vitritis. TB should have choroidal granulomas. CMV in the setting of HIV usually starts in the periphery, has “pizza pie” retina, very white necrosis and yellow borders with heme in center zones, and not the disk in particular like in this patient. Severe hypertension would have more cotton wool spots, bilateral, and flame heme along arcades. CSD due to B. henselae usually begins with a cutaneous lesion at the inoculation site and evolves through vesicular, erythematous, and papular phases. Painful regional lymphadenopathy in the drainage of the lesion together with fever are the hallmarks of CSD. Ocular manifestations of CSD include Parinaud's oculoglandular syndrome, neuroretinitis, papillitis, optic neuritis, and focal retinochoroiditis. In the USA, CSD causes approximately 24,000 cases annually (mainly in children) with neuroretinitis in about 2%. In 53 patients (62 eyes) with CSD neuroretinitis: 67% of patients had a history of a cat scratch, macular star developed in 28 eyes (45%) and bilateral lesions were detected in 17% (9 patients). Only 5 patients had significant visual complications that did not resolve quickly [Ophthalmology. 2012 Jan;119(1):183-7]. Initial good visual acuity and absence of systemic symptoms was associated with favorable visual outcomes. CSD is well described in Latin America though other cause of neuroretinitis are more important than in developed countries like the US. In Perú, proven CSD in Lima was described in 12 patients with fever, malaise, and lymphadenopathy – none had ocular lesions [Rev Inst Med Trop Sao Paulo. 2002 Nov-Dec;44(6):325-30]. Our patient received 4 weeks of doxycycline plus rifampin and recovered 70% of her vision [Image C] and will be continued for at least 2 more weeks pending re-examination. Special thanks to Instituto Nacional de Oftalmologia (INO) of Lima and Dra. Betty Campos/Dra. Amelia Cerrate and to Dr. Mark Paris and Robert Raden in Florida. |
 Discussion: An IgG/M ELISA for Bartonella henselae was positive at 62 units (positive >15). Other infectious causes of stellate maculopathy secondary to severe neuroretinitis were ruled out as follows: chest X-ray normal and PPD negative; VDRL and FTA abs negative; IgM toxoplasmosis negative and IgG toxoplasmosis positive; IgG-CMV positive; Salmonella and Brucella serology negative. Outside opthalmologists had given a diagnosis of diabetic retinopathy, despite normal glucose levels, and toxoplasmosis, despite negative IgM and high titred IgG suggestive of remote infection. Much more unusual causes of neuroretinitis are histoplasmosis, Toxocara, Herpes zoster, lyme, leptospirosis and parotiditis.
Discussion: An IgG/M ELISA for Bartonella henselae was positive at 62 units (positive >15). Other infectious causes of stellate maculopathy secondary to severe neuroretinitis were ruled out as follows: chest X-ray normal and PPD negative; VDRL and FTA abs negative; IgM toxoplasmosis negative and IgG toxoplasmosis positive; IgG-CMV positive; Salmonella and Brucella serology negative. Outside opthalmologists had given a diagnosis of diabetic retinopathy, despite normal glucose levels, and toxoplasmosis, despite negative IgM and high titred IgG suggestive of remote infection. Much more unusual causes of neuroretinitis are histoplasmosis, Toxocara, Herpes zoster, lyme, leptospirosis and parotiditis.