 |
2013 Case #8 |  |
|
Here is another case seen by participants during the last week of the 9-week Diploma Course when the class was on a 4-day field trip to Iquitos, Perú on the banks of the Amazon River. Iquitos, with a population of approximately 400,000, is the largest city in the world that can only be reached by air or by river. The nearest road ends over 400 km away. One final case seen in Iquitos will be presented next week and will be the last we share from the 2013 Gorgas Diploma Course. |
|
The following patient was seen in the inpatient department at Iquitos Hospital. |
|
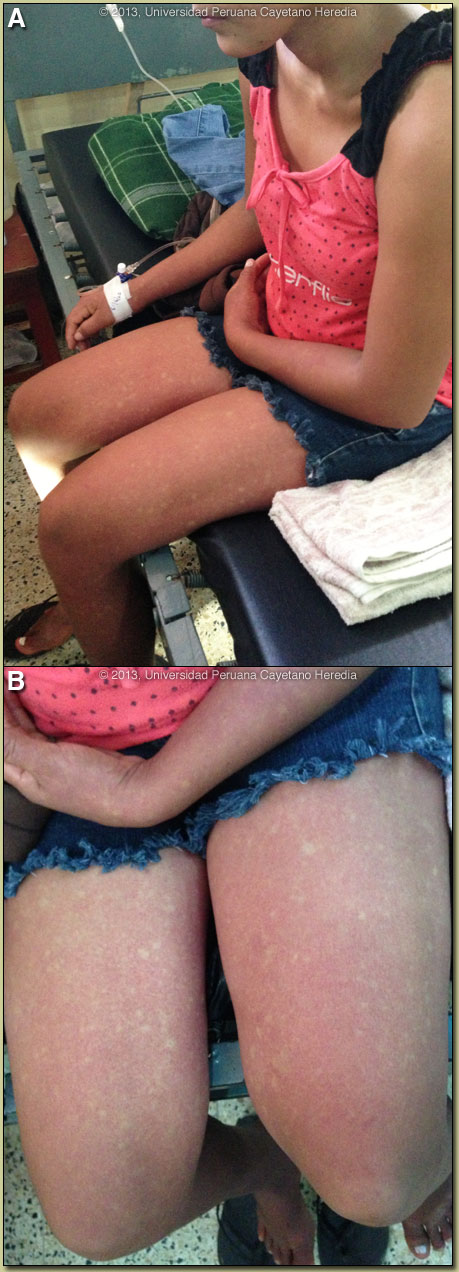
Epidemiology: Lives and grew up in urbanized areas of Iquitos. No febrile illnesses in the family. No known TB exposure. She is sexually active. Physical Examination: Afebrile; normal vital signs. HEENT: mucosa clear, no mucosal bleeding, no lymphadenopathy. Chest: clear. Abdomen: no hepatosplenomegaly. Skin: see Images A and B. Neurological: normal. Laboratory Results: Hb: 13.4; Hematocrit: 40; Platelets: 32,000; WBC: 6800 (38 neutrophils; 56 lymphs). Glucose: 94; Creat: 0.86 (N). Urinalysis normal.
|
| Diagnosis: Dengue. |
|
Discussion: PCR positive for dengue serotype 2. Tourniquet test was positive. A positive tourniquet test occurs in up to 50% of patients with classic dengue and in almost all patients with severe dengue. A positive tourniquet by itself may be positive with a number of other infections so is not diagnostic of dengue by itself. Virus may be isolated from blood; PCR of blood will be positive, or NS1 antigen may be detected in the blood during the first 5 days only. IgM elevations do not occur until 5 days or more, so a sample taken earlier may be negative. Four-fold elevations of IgG on acute and convalescent serum may be required to confirm diagnosis. Dengue infections range from asymptomatic through a range of clinical manifestations to death. The incubation period of this flavivirus is normally 3–7 days from the time of the infective bite of the Aedes mosquito and 14 days at the most. After the incubation period, the illness begins abruptly and is followed by the three phases – febrile, critical and recovery. Typical dengue fever is manifest by frontal headache, retro-orbital pain, muscle and joint pain, nausea, vomiting and rash. The febrile phase lasts 2–7 days. An early flush-like rash often occurs and wanes after a few days to be replaced by a morbilliform rash that is often described as white islands on a red sea (as in our patient Image A and B). A late petechial rash may also occur. A diagnosis cannot be made on clinical findings alone. Malaria, other arboviruses, leptospirosis, rickettsial disease, measles, rubella, or typhoid may present similar findings in the pre-rash phase of infection and need to be tested for. Mild elevations of liver function tests are typical of dengue as well as the other diseases mentioned. The morbilliform rash is similar to that found in rubella, which needs to be considered in inadequately immunized patients. If symptoms begin more than 2 weeks after a patient has left an endemic area dengue can be essentially ruled out. When the temperature drops to 37.5–38.0ºC or less and remains below this level – usually on days 3–7 of illness – an increase in capillary permeability in parallel with increasing haematocrit levels may occur, and marks the beginning of the critical phase when it occurs (though not in this case) [see Gorgas Case 2011-09 for an example]. This period of clinically significant plasma leakage usually lasts 24–48 hours. Plasma leakage, haemoconcentration and abnormalities in homeostasis characterize severe dengue when it occurs. The mechanisms leading to severe illness are not well defined but the immune response, the genetic background of the individual and the virus characteristics may all contribute to severe dengue. Mild bleeding such as epistaxis or mucosal bleeding by itself is not enough to classify a patient as severe dengue. Increasingly, small pleural effusions are recognized in dengue by ultrasound but are not indicative of severe plasma leakage unless there is respiratory compromise. Primary infection by any of the four virus serotypes (DEN 1-4) is thought to induce lifelong protective immunity to the infecting serotype. Sero-epidemiological studies in Cuba and Thailand consistently support the role of secondary heterotypic infection (with another serotype) as a risk factor for severe dengue, although there are a number of reports of severe cases associated with primary infection, which may be a reflection of viral virulence factors. Dengue was reported in Perú for the first time in 1990; since then, all four serotypes are circulating, mainly along the north coast and the jungle. Lima was affected for the first time in 2005, with 200 cases of serotype 3 diagnosed in the northern suburban district of Comas. The Aedes vector remains present in isolated areas of the city and 45 cases were reported from Lima in 2012; most of them were imported cases. During 2012, 23,857 probable cases of dengue with no warning signs have been reported nationwide; 4,606 additional probable cases with warning signs were also reported, and 195 cases (0.7%) presented with severe dengue. Almost 90% of these cases were reported from the departments of Ucayali and Loreto. Up to February 2013, 5,290 probable cases have been reported; 80% of these cases did not have warning signs and most of them came from Ucayali. A new serotype, DEN-2 Asian-American variant, was isolated in 2011 for the first time and appears to be persisting. Our patient was treated with paracetamol and intravenous hydration. The rash is beginning to fade but is still very noticeable several days after admission. |