 |
Gorgas Case 2022-06 |
|
The following patient was seen at the Dermatology Clinic of the Hospital Nacional Cayetano Heredia, Lima, Peru by Dr. Francisco Bravo. We would like to thank him for his assistance and input in this case.  History: A 66-year-old male patient presented with a 10-day history of fever, malaise, muscle weakness, pain, and an erythematous patch on his right thigh. 8 days prior to presentation, the lesion in the thigh ulcerated, forming a black scab with surrounding lymphangitis (Image A), and he noticed multiple itchy and purpuric papular lesions on all four extremities. Epidemiology: He traveled to the Limpopo province in northern South Africa for a week-long hunting safari, returning one week before presentation. He was not taking malaria prophylaxis. Three days after his arrival in South Africa, one day before symptoms started, he found a small tick on his right thigh, which he removed after manipulating it. Physical Examination: Vital signs were within normal limits, with no fever. Skin: Black scab, about 1cm in diameter, with surrounding erythema and lymphangitis in the inner right thigh (Image B), with a diffuse maculopapular rash in arms and legs (Image C). The rest of the physical exam was non-contributory. Laboratory: Hb 15.9 mg/dL, Hct 46.2%, Leu 4 000 (15% bands, 57% segmented, 20% lympho, 4% mono, 2% eos, 2% baso), 165 platelets. ALT 57, AST 41, AlkPhos 20, GGTP 16.2. Thick smear for malaria was negative..
|
|
Diagnosis: African tick-bite fever (Rickettsia africae) 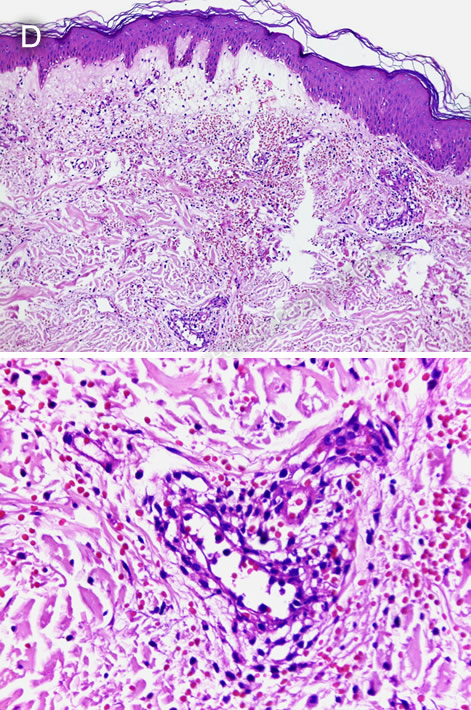
 Discussion: The diagnosis of ATBF must be made clinically due to the time needed to get laboratory confirmation. Eschar, compatible rash, flulike symptoms and travel to game parks of Southern Africa is an indication for immediate oral doxycycline to which the patients usually respond in less than 1 day. A local serum panel for Rickettsial infections (including R. conorii, R. typhus, R. prowazekii, and R. rickettsia) was negative. Leg skin biopsy samples were sent to the United States National Institutes of Health for further testing; immunohistochemistry was reactive for spotted fever group Rickettsia species and PCR was positive for Rickettsia spp. A skin biopsy revealed coagulative necrosis and vasculitis, with lymphocytic inflammatory infiltrates, extravasation of red blood cells, and small thrombi (Image D). Rickettsiae are small arthropod-borne gram-negative intracellular coccobacilli of worldwide distribution. They are typically arranged into three groups based on their physiological characteristics. The spotted fever group includes tick-transmitted rickettsioses such as Rocky Mountain Spotted Fever (R. rickettsia), ATBF (R. africae), Mediterranean spotted fever (R. conorii), Siberian tick typhus (R. sibirica), Queensland tick typhus (R. australis), among others. The typhus group includes murine typhus (caused by R. typhi) and louse-borne epidemic typhus (caused by R. prowazekii). Finally, Orientia tsutsugamushi, the causal agent of scrub typhus, has several structural differences from the other two groups, and thus is considered a third separate group. ATBF is caused by transmission of R. africae through the bite of Amblyomma hebraeum and Amblyomma variegatum ticks, which also serve as reservoirs. It usually presents as a mild illness. A recent systematic review found that almost 90% of patients presented with fever, 39% with a single eschar and 47% with multiple eschars, 51% with regional lymphadenopathy, and 42% with rash (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8805502/). A. hebraeum is present in rural areas of central, east, and west Africa, and in the eastern Caribbean, while A. variegatum is present in southern Africa (https://pubmed.ncbi.nlm.nih.gov/12954562/). Both species are known for their aggressive behavior, with patients often noting multiple bites from different ticks in their lower limbs. There are few reported autochthonous cases in Southern Africa; underreporting may be due to the mild course of the disease, infection at early ages, or difficulty identifying the eschar in darkly pigmented people. In returned travelers, which account for 90% of ATBF cases, the most reported country of travel among confirmed cases is South Africa, with far less cases reported in travelers from Swaziland, Zimbabwe, Tanzania, Ethiopia, Kenya, Uganda, and Guadeloupe (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8805502/). Definitive diagnosis of g ATBF, as with other rickettsioses, is challenging and not usually necessary if the presentation is classic; rapid response to doxycycline also provides rapid confirmation. Blood or tissue cultures, while helpful if positive, require using complicated cell culture technique and may pose a risk to laboratory personnel, thus requiring a Biosafety Level 3 laboratory. Similarly, immunohistochemistry and PCR of eschar or skin biopsies are useful but rarely available. Serologic tests are more readily accessible and commonly used for diagnosis: a fourfold increase in titer from acute- and convalescent-phase sera in indirect immunofluorescence assay is considered confirmatory. However, group-specific antigens are cross-reactive and therefore a species-specific diagnosis cannot be made this way. The differential diagnosis of ATBF depends on the clinical presentation. The non-specific prodromic phase with fever and headaches can be confused with malaria or any other febrile illness from the tropics. An eschar may be similar to some insect bites or skin trauma. Skin rashes may be indistinguishable from those seen in rubella, measles, syphilis, gonococcemia, leptospirosis, typhoid, or drug reactions. The combination of the fever, eschar and rash plus the history of travel to an endemic area make the diagnosis of ATBF more likely. Doxycycline is the treatment of choice, usually 100 mg twice daily for 5-7 days,with near universal cure. If IV doxycycline is not available, IV fluoroquinolones may be used for critically ill patients who cannot tolerate oral medication. Pre- or post-tick antibiotic prophylaxis is not recommended; people in endemic areas should be advised to apply DEET periodically and examine themselves for attached ticks daily. Treating dogs and the environment with parasiticides may also reduce the burden of local disease. Our patient was treated with doxycycline for 7 days starting 10 days after symptom onset, with rapid improvement of the systemic symptoms, and progressive resolution of the skin lesion. |