 |
Gorgas Case 2022-07 |
|
The following patient was seen as an outpatient at the Tropical Medicine Institute at Cayetano Heredia Hospital by the 2022 Gorgas Course participants.  History: A 65-year-old male patient noticed the appearance of erythematous painful nodules in his thorax, abdominal skin and upper limbs, and fever that was treated symptomatically at the beginning of 2019. By mid-2019, the symptoms persisted, and some nodules ulcerated and started draining a purulent secretion. In March 2020, a week before the COVID-19 confinement, he was seen in our hospital, received some therapy which he does not remember, and went back to the jungle, where he improved completely with the therapy. He remained asymptomatic until March 2022, when he received the influenza vaccine and on the following day woke up with general malaise. On the next day he noticed the appearance of painful erythematous subcutaneous nodular lesions in his left submandibular area. He was prescribed symptomatic treatment and antibiotics which he took without improvement. On the following days he experienced bilateral paresthesiae on his hands, posterior and anteromedial aspects of forearms, and feet. He also had a cold sensation on his hands and feet. On the following days the subcutaneous nodules progressively involved his neck, face, chest, back, abdomen, and upper limbs, and he developed fever. Some of the nodules became ulcerated (Images A and B). Epidemiology: He was born and lives in Ucayali, in the jungle of Peru. He works operating heavy machinery. Reports having been bitten by leeches several times. No known TB contacts. Physical Examination: Afebrile. BP: 105/70 mmHg. HR: 72 bpm. RR: 16 rpm. Sat: 97 % (FiO2: 0.21). Skin: Multiple dermal and subcutaneous erythematous nodular lesions, mobile, tender to palpation, of varying size, localized on the face, neck, over the upper limbs, anterior and posterior thorax and abdomen, and thighs, some of these have pustules on the top, crusts or are ulcerated Images C-G). Lungs: clear to auscultation bilaterally. Cardiovascular: regular heartbeat, no murmurs. Abdomen: normal bowel sounds, soft, non-distended, no tenderness to palpation. No costovertebral angle tenderness. Neurological: thickened superficial branch of the right ulnar nerve, terminal branch of the left radial nerve, both common peroneal and posterior tibial nerves plus hypoesthesia in both hands with anesthesia in the right ulnar area and on both feet. Decreased muscle strength in both cubital territories. Cranial nerves: afferent corneal sensation decreased bilaterally.
|
|
Diagnosis: Mycobacterium leprae. Type 2 leprosy reaction. Treated lepromatous leprosy (LL). 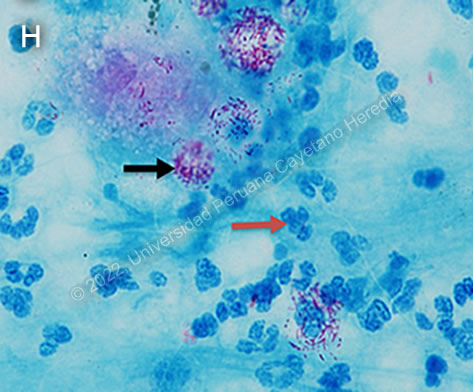
 Discussion: When first seen by us 2 years earlier, he presented with areas of infiltrated skin all over the body, as well as tender dermal and subcutaneous nodules on the upper limbs, thorax, abdomen and thighs characteristic of lepromatous leprosy with type 2 reaction (lesions of erythema nodosum leprosum). He was treated with a complete course of WHO multi-drug therapy (MDT) for 1 year plus thalidomide. Patients with lepromatous leprosy have no cell-mediated immunity against the bacterium, so the bacteria are killed after one year of therapy, but they remain in the body because these patients cannot eliminate them; they will disappear progressively over several years. Leprosy is a disease of peripheral nerves and skin. Leprosy can be diagnosed clinically in any patient with simultaneous skin lesions and sensory loss over the lesions unless there is hyperkeratosis. The most common presentation of type 2 inflammatory reactions is erythema nodosum leprosum (ENL). ENL may occur in patients prior to therapy as in this case, during therapy, and/or after therapy until the antigen load decreases markedly. ENL may present as repeated acute episodes or may be chronic and ongoing. This is a systemic immune-mediated disorder, associated with antigen-antibody immune-complex deposition in tissues, usually with high levels of tissue and circulating TNF-alpha. Lepromatous patients have high levels of antibodies and high levels of antigens (bacterial load) and they produce immune complexes. ENL presents usually with many tender dermal and subcutaneous erythematous nodules that occurs in up to 50% of lepromatous leprosy cases [Am J Trop Med Hyg. 2006;74:868-79] and 25% of borderline lepromatous patients [Dermatology Online J 2006; 12:29], due to their high bacterial loads. The lesions of ENL differ from the common erythema nodosum in that the nodules occur anywhere in the body rather than on the shins, whereas in erythema nodosum they occur on the shins and rarely in other places. On the shins, erythema nodosum lesions are difficult to hold, they are more plaque-like, whereas ENL lesions in other areas are easily hold as a subcutaneous nodular lesion. In addition, ENL nodules may ulcerate and drain pus, with no pyogenic bacteria but with usually dead leprosy bacilli, a feature that does not occur in the common erythema nodosum. The PAP smear of the content of the nodules usually shows a hypocellular smear composed mainly of neutrophils with abundant bacilli on Fite-Faraco staining (Image H). As long as patients have bacteria (antigens), they produce immune complexes and may precipitate ENL repeatedly several years after therapy. Clinically, a relapse would not be suspected in this patient, due to lack of new infiltrative areas on the skin and no new peripheral nerve involvement, so he only needs therapy for the reaction. ENL histopathology shows an infiltration by neutrophils, which is not seen in a biopsy of leprosy without type 2 reaction. ENL may also produce, to varying degrees, fever, neuritis, edema, arthralgias, leukocytosis, uveitis, dactylitis, myositis, periostitis, orchitis, lymphadenitis and nephritis. ENL can be treated symptomatically if mild or with prednisone or thalidomide if severe. Thalidomide is the drug of choice for severe ENL as in this case and very effective for neuritis due to type 2 reaction. A dose of 300 to 400 mg daily will usually control the reaction within 48 hours. The dose is then tapered usually every 7-10 days to a maintenance level, which is generally around 100 mg daily and then attempts are made to taper off the drug. This patient had been having persistent ENL for 3 months. Uncontrolled ENL can lead to secondary amyloidosis. In cases of difficult to treat ENL, some drugs reported as useful have been azathioprine [J Clin Diag Res 2017;11:FD01] minocycline [JAMA Dermatol 2015;151:1026], and etanercept [Ann Bras Dermatol 2017;92:575 and Clin Infect Dis 2011;52:e133]. |