| 2005 Case #9 |  |
|
| The following patient was seen by course participants on the 36-bed inpatient unit of the Tropical Medicine Institute. |
 History: 27 yo male who developed an erythematous lesion developed over the left thigh 3 weeks after closed trauma with an axe 4 years ago. Over the next year the lesion evolved with marked edema, erythema, and multiple fistulas draining dark brown purulent material without any granules noted which have persisted to the present. No treatment had been attempted prior to the current presentation. Otherwise healthy with no past medical history. History: 27 yo male who developed an erythematous lesion developed over the left thigh 3 weeks after closed trauma with an axe 4 years ago. Over the next year the lesion evolved with marked edema, erythema, and multiple fistulas draining dark brown purulent material without any granules noted which have persisted to the present. No treatment had been attempted prior to the current presentation. Otherwise healthy with no past medical history.
Epidemiology: Farmer born and living in the jungle regions of Ayacucho Department. Physical Examination: Afebrile, normal vital signs. No organomegaly or lymphadenopathy. Thigh lesions and draining fistulas are shown in Image A and B. Laboratory Examination: Hct. 39%, WBC 11,400 (72% neutrophils, 11% eos). Normal liver function. Stool exam positive for Strongyloides. Chest X-ray normal. X-ray of the thigh and leg showed no evidence of osteomyelitis or arthritis. A biopsy was obtained. |
| Diagnosis: Actinomycosis. |
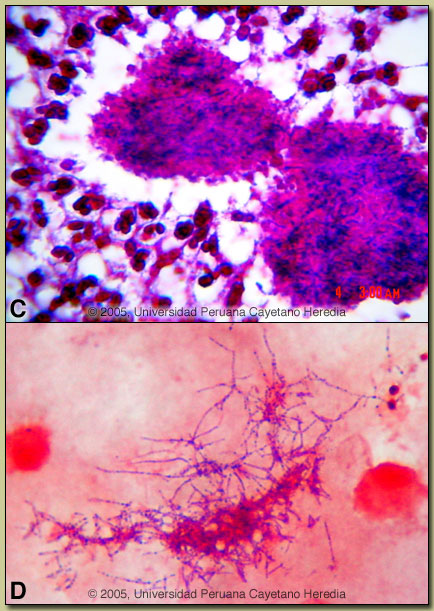 Discussion: A deep incisional biopsy of soft tissue was performed. Histopathology demonstrated acute and chronic inflammatory reaction and typical sulfur granules of actinomycosis [Image C]. A Gram positive filamentous bacilli was isolated in an anaerobic culture [Image D]. The Ziehl-Neelsen stain of the cultured organism was negative and the growth under strict anaerobic conditions rules out Nocardia indicating the organism to be Actinomyces species. Agents of eumycetoma (maduramycosis) would have resulted in broad branching hyphae being found on histolology. Speciation of the actinomyces requires sophisticated testing not available at our institute. Discussion: A deep incisional biopsy of soft tissue was performed. Histopathology demonstrated acute and chronic inflammatory reaction and typical sulfur granules of actinomycosis [Image C]. A Gram positive filamentous bacilli was isolated in an anaerobic culture [Image D]. The Ziehl-Neelsen stain of the cultured organism was negative and the growth under strict anaerobic conditions rules out Nocardia indicating the organism to be Actinomyces species. Agents of eumycetoma (maduramycosis) would have resulted in broad branching hyphae being found on histolology. Speciation of the actinomyces requires sophisticated testing not available at our institute.
Primary cutaneous actinomycosis is an uncommon entity [Trans R Soc Trop Med Hyg. 2004 Jan;98(1):3-11]. Actinomycetes are generally thought to be an endogenous human organism colonizing the oro-pharynx, gastrointestinal, and female genitourinary tracts, and producing disease via local extension from these foci. Periodic case reports of primary cutaneous infection appear and this is the second such case seen during the Gorgas Course in Peru in the past 5 years [see Gorgas Case 2001-09]. The main and important differential diagnosis in this case is maduramycosis (e.g., Madura foot) [see Gorgas Case 2002-04]. Other diagnoses in the differential include TB, botrymycosis (chronic staphylococcal infection) [see Gorgas Case 2003-04], and malignancy. Maduromycosis is a common subcutaneous mycosis in the tropics and is caused by a wide variety of fungal organisms. In maduromycosis, the granules usually come to the surface spontaneously, unlike in this case, where there was copious drainage from the fistulous tracts without granules. In contrast to bacteria and actinomycosis (which is responsive to Penicillin and other antibiotics), they are poorly responsive to medical therapy and usually require aggressive surgery or amputation. Other subcutaneous mycoses to think of in the tropics include sporotrichosis, chromomycosis, and lobomycosis (phaeohyphomycosis). Our patient was begun on TMP-SXT and amikacin prior to obtaining the microbiological diagnosis of actinomycosis. In general, high dose intravenous penicillin for 6 weeks followed on chronic oral therapy for at least one year is the treatment of choice for subcutaneous actinomycosis. The patient also received thiabendazole for his strongyloidiasis. |