Clinical History:
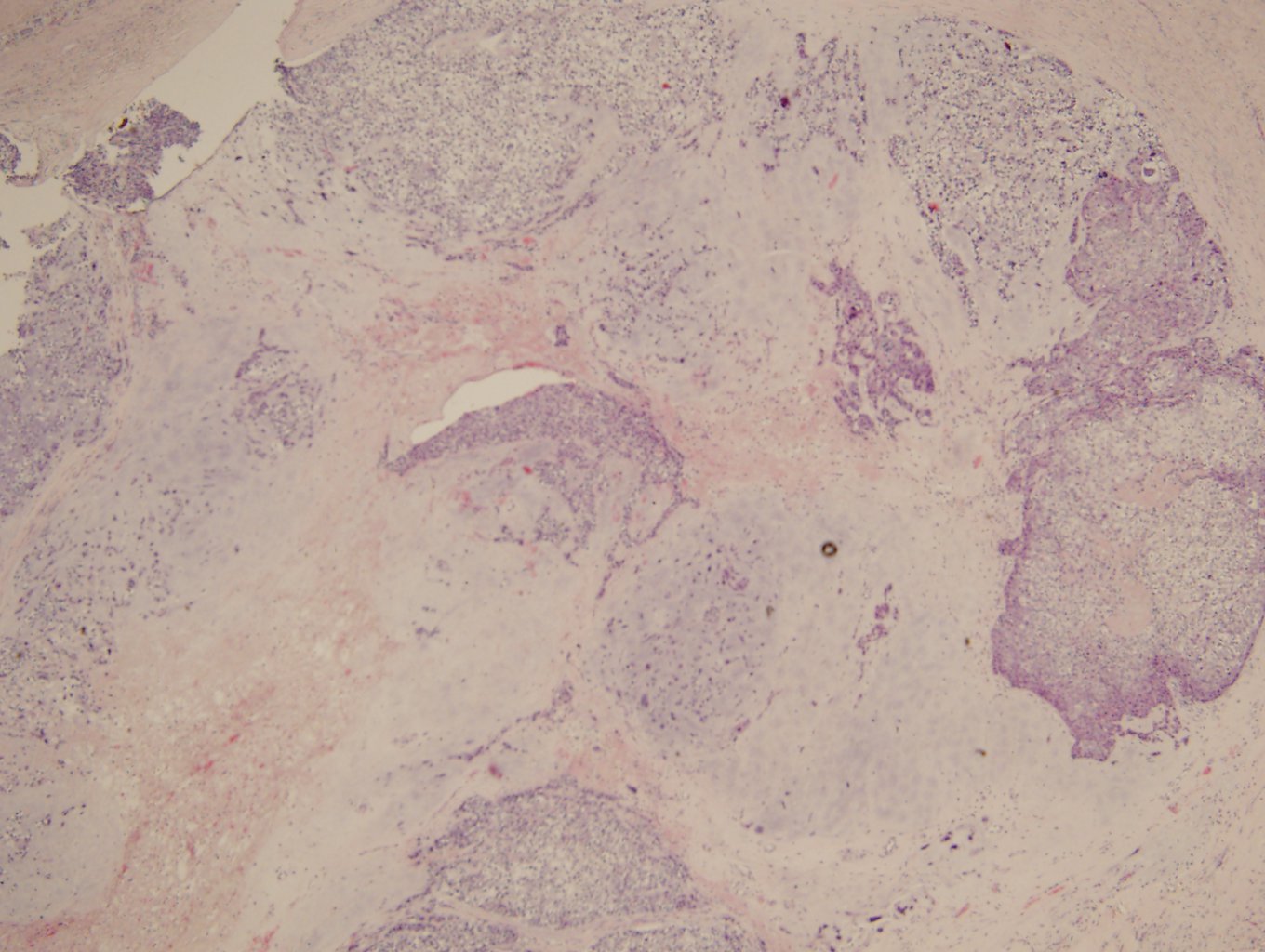
44 year old male with pleural rind biopsy
|
Choose the correct diagnosis:
|
The answer is “D”, NUT midline carcinoma.
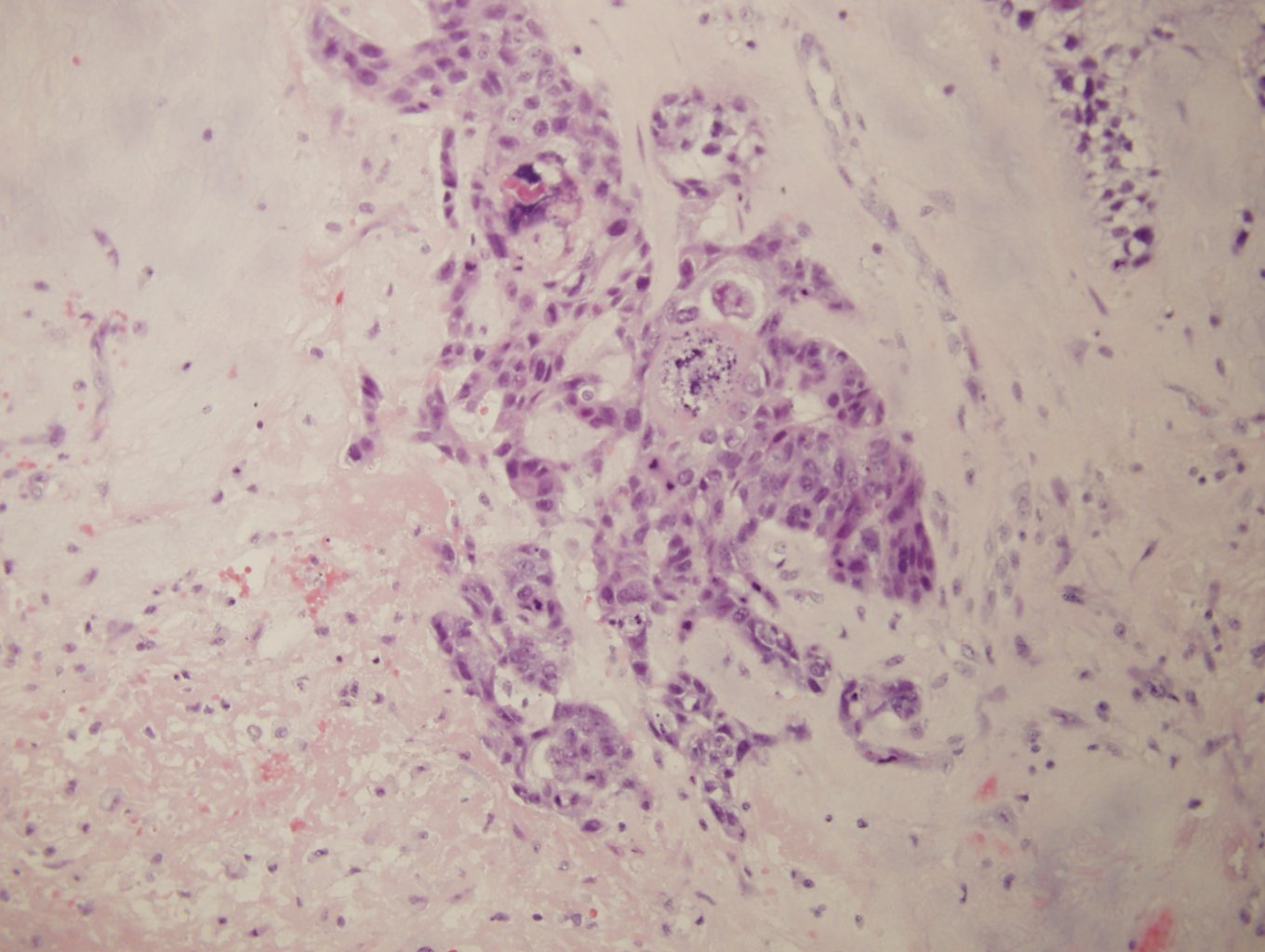
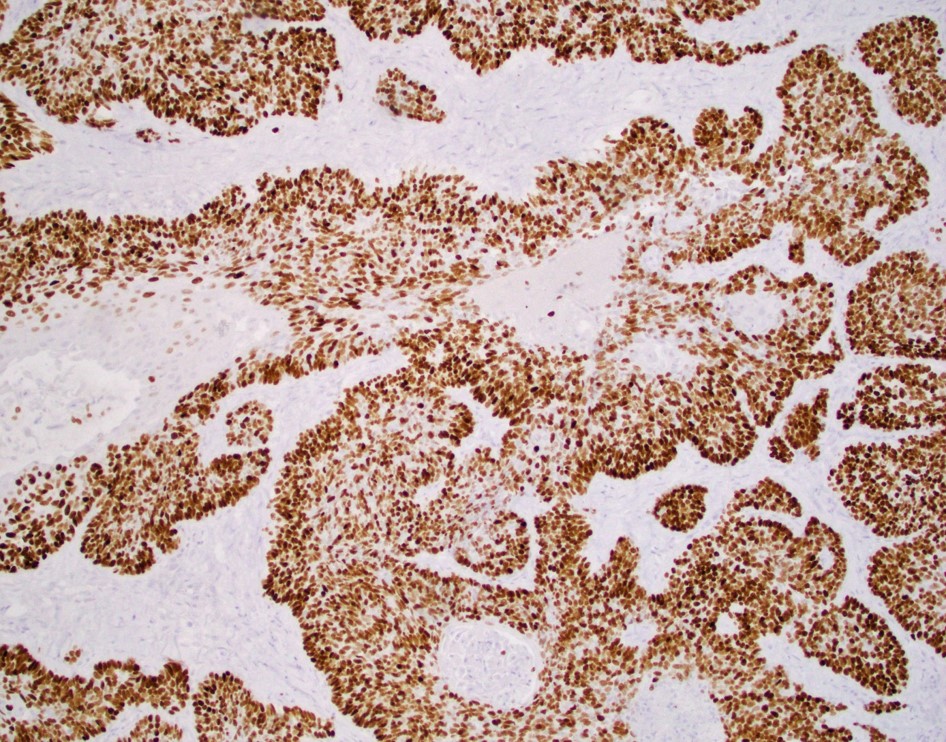
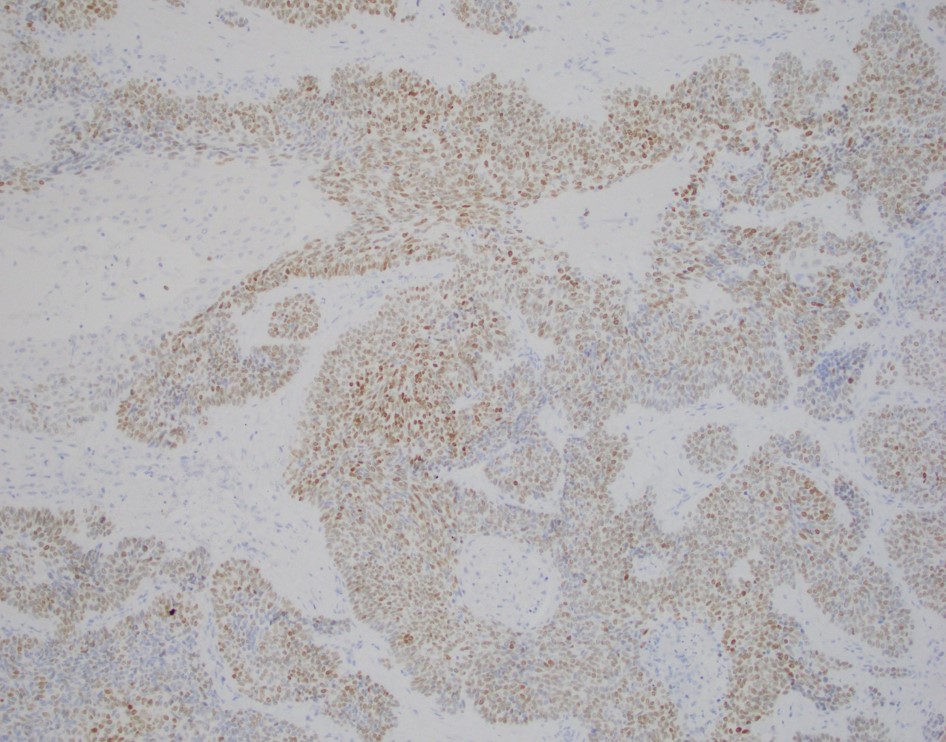
NUT midline carcinomas (NMC) are a subtype of squamous cell carcinoma carrying fusions of the NUT (nuclear protein in testis) gene on chromosome 15 to either BRD4 on chromosome 19 or less commonly the BRD3 (9q34.2) gene. NMC typically afflicts younger patients, and most commonly arises in midline structures of head and neck and mediastinum, but cases involving the urinary bladder, pancreas, adrenal gland, kidney and salivary gland have been described. Histologically, NMC is a primitive appearing carcinoma with areas of “abrupt” transition to keratinous differentiation. It is highly lethal, with a median survival time of 6.7 months. An antibody to the NUT protein has been developed and is highly specific for NMC. NMC express squamous markers p40 and p63 and about half of cases express CD34. Neuroendocrine markers are negative and there has been no evidence of EBV or HPV infection in NMC. BRD4 and BRD3 are members of the BET family of chromatin readers. TheNUT-BRD4 fusion acts to block differentiation to preserve a stem cell-like nature of the neoplastic cells. There is no established treatment for NMC, although various chemotherapy and radiation therapies are typically used. Recently, bromodomain (BET) inhibitors have been used with some success in NMC.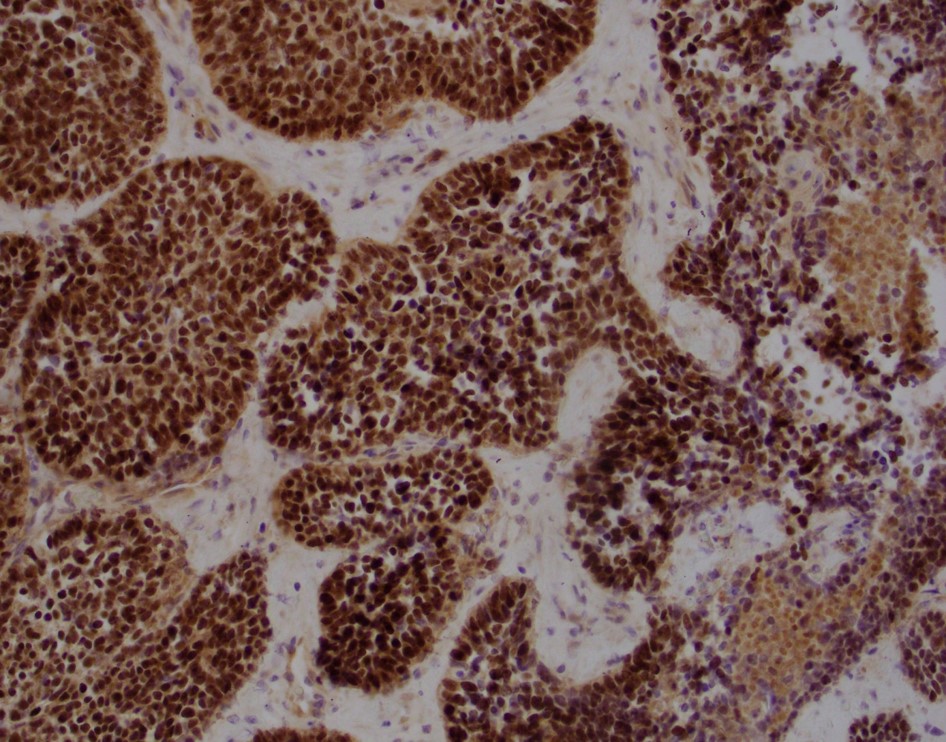 NUTM1-BRD4 fusion was identified by Next-gen sequencing
NUTM1-BRD4 fusion was identified by Next-gen sequencing
References
French C. NUT midline carcinoma. Nature Reviews. 2014. Doi: 10.1038/nrc3659
Stelow EB. A review of NUT midline carcinoma. Head and Neck Pathology. 2011; 5 (1): 31-35.
Contributed by Dr. Todd Stevens