Clinical History:
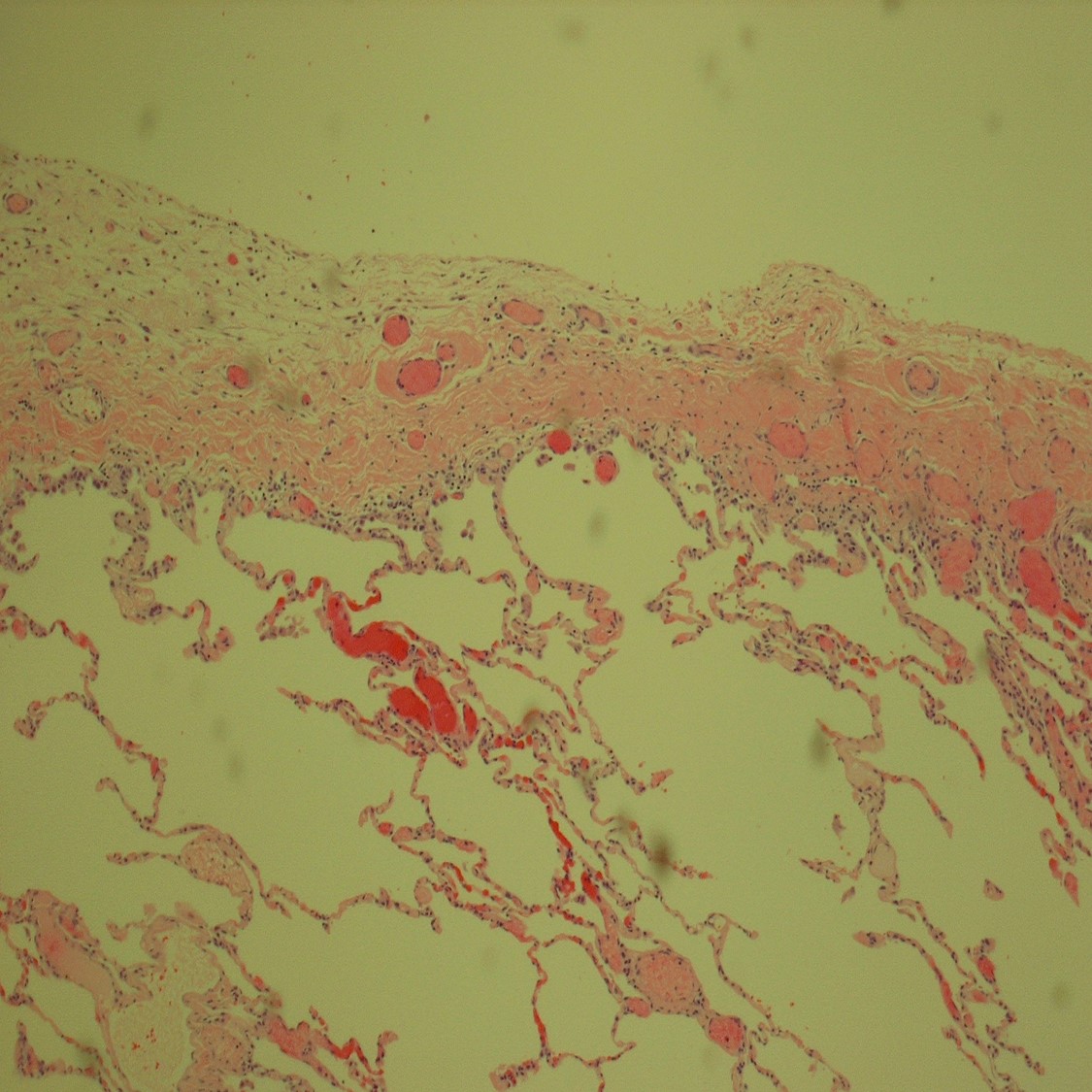
This 39-year-old Hispanic woman, a never smoker, underwent thoracotomy and pleurodesis for spontaneous pneumothorax in 2012. A subsequent pneumothorax in 2014 resulted in a right upper lobe wedge biopsy (shown). She is asymptomatic except for shortness of breath when exposed to cigarette smoke. Recent radiographs show bilateral pulmonary cysts and new renal masses.
Which is the correct diagnosis?
- Chronic obstructive pulmonary disease (COPD)
- Adult polycystic kidney disease
- Birt-Hogg-Dube syndrome
- Lymphangioleiomyomatosis (LAM)
The answer is “C”, Birt-Hogg-Dube syndrome.
Discussion
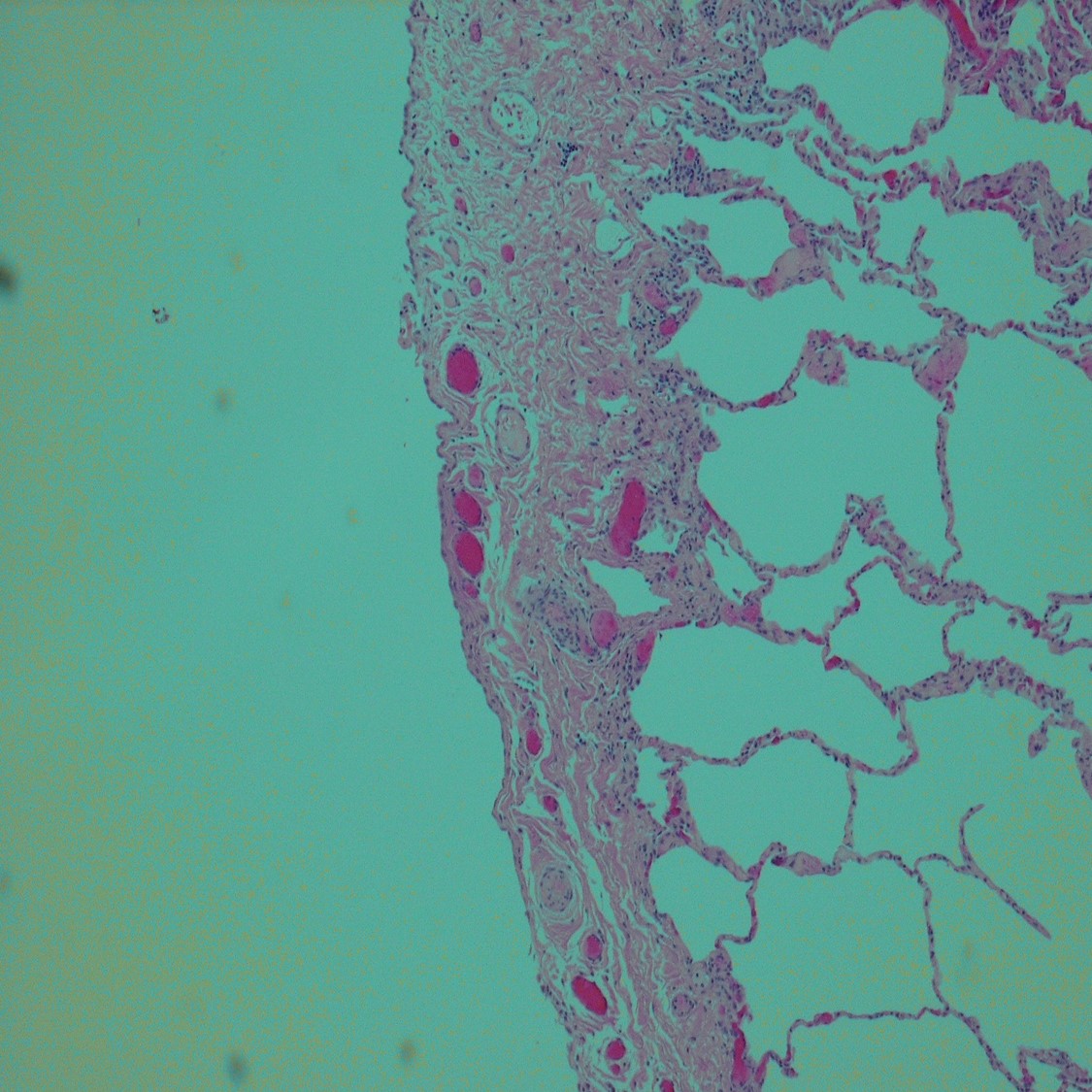
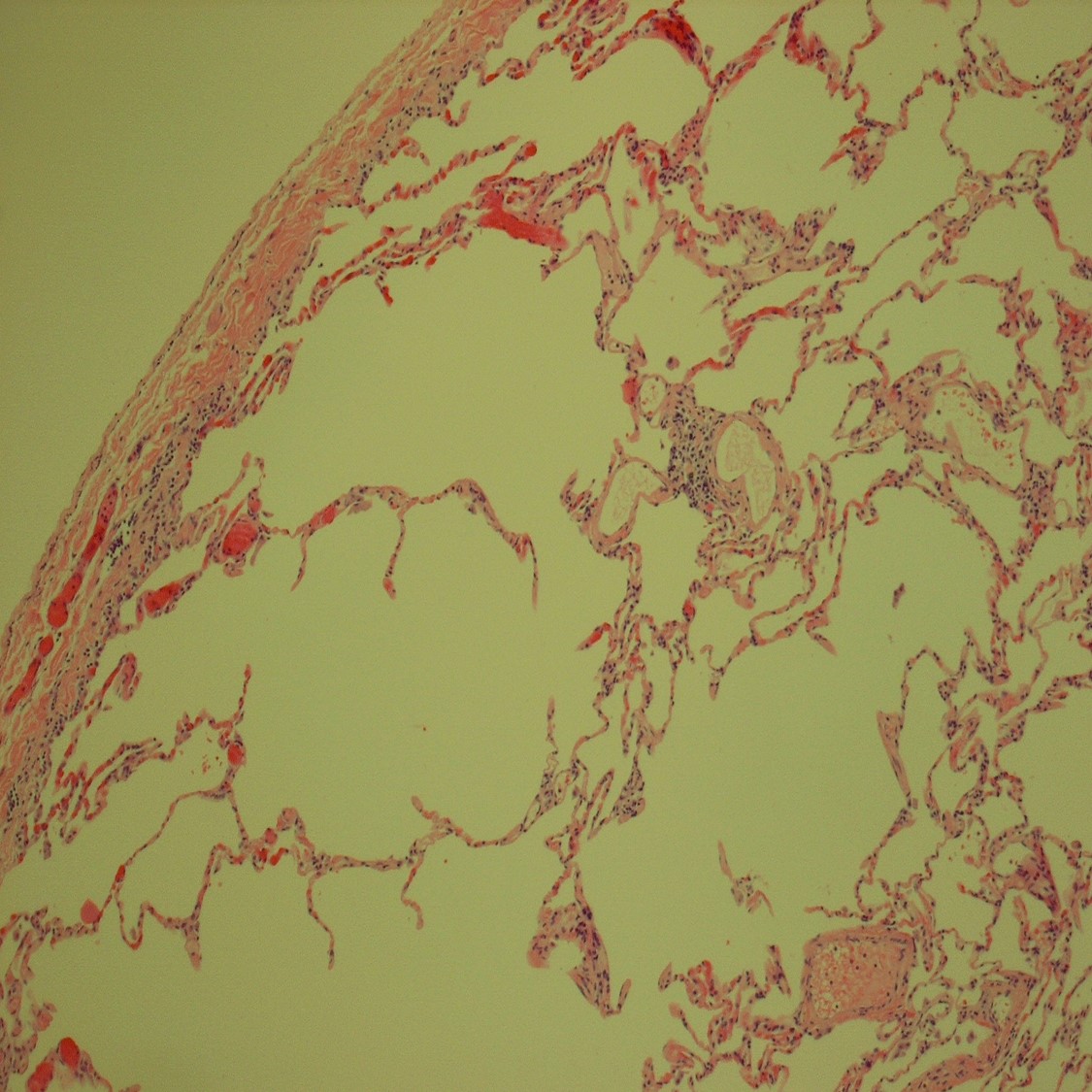
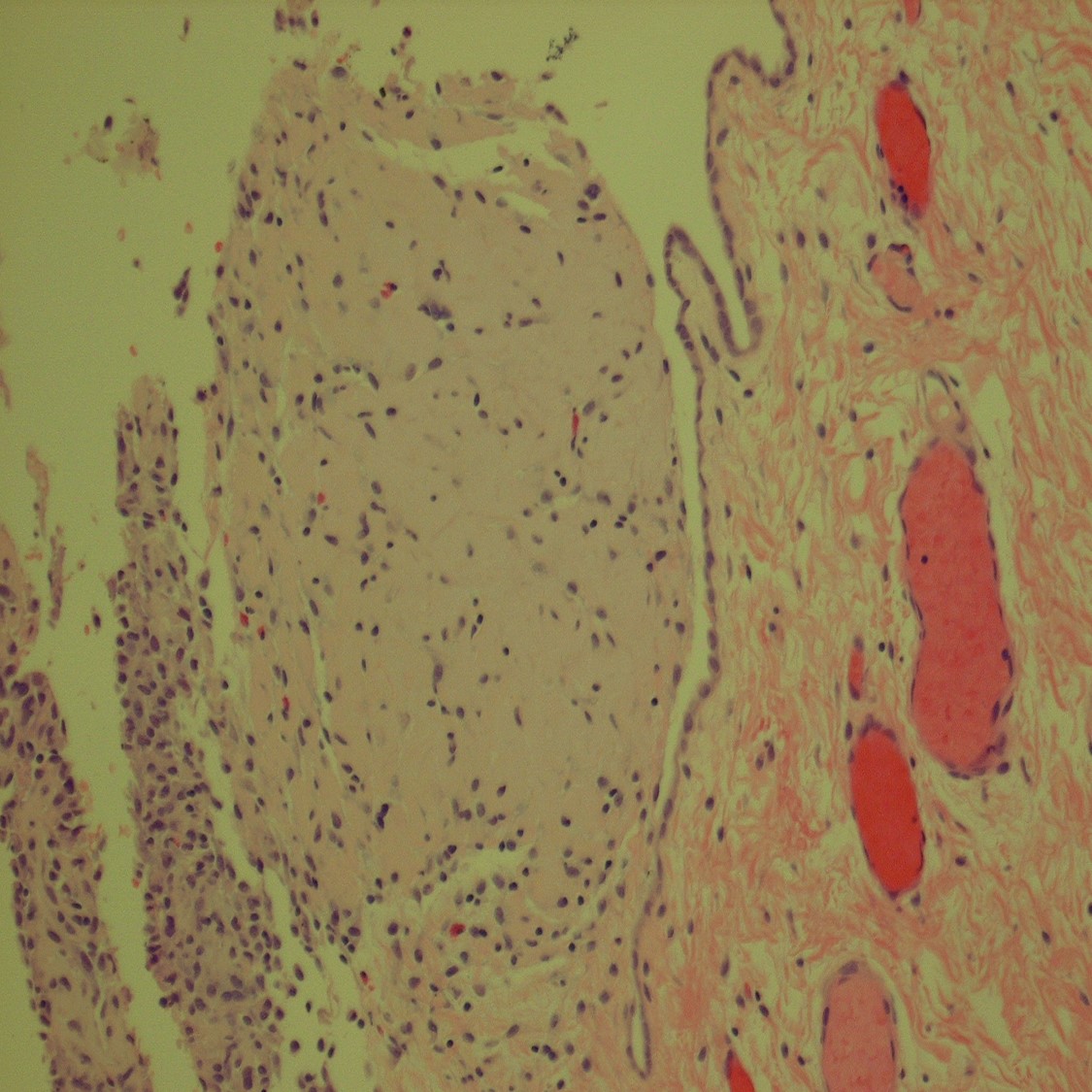
The slides show bland lung parenchyma except for mild cystic dilation of subpleural airspaces. The pleura is slightly thickened but is also generally bland, except for focal fibrosis and reactive mesothelial cell hyperplasia (fourth slide), possibly the result of the previous pleurodesis. No significant inflammation or atypical features are seen.
Birt-Hogg-Dube is an autosomal dominant genetic disorder associated with mutation in the FLCN gene which codes for the protein folliculin. It is characterized primarily by benign dermal appendageal tumors (fibrofolliculomas), subpleural pulmonary cysts, and markedly increased incidence of renal neoplasms (primarily oncocytomas and chromophobe carcinomas). Patterns of expression vary but can be relatively constant in affected families. Diagnosis is confirmed by genetic testing.
References
- Birt, A. R.; Hogg, GR; Dubé, WJ (1977), "Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons", Archives of Dermatology, 113(12): 1674–7, doi:10.1001/archderm.113.12.1674, PMID 596896
- Ayo, Dereje S.; Aughenbaugh, GL; Yi, ES; Hand, JL; Ryu, JH (2007), "Cystic Lung Disease in Birt-Hogg-Dubé Syndrome", Chest, 132(2): 679–84, doi:10.1378/chest.07-0042, PMID 17505035
Case contributed by Ralph Crowe, M.D., , Professor, Anatomic Pathology, UAB Pathology