Clinical History
The patient is a 73-year-old male with prostate cancer, HTN, hyperlipidemia and PE. Laboratory data from the outside hospital included: Cr 1.3, 24 hr protein 516, C3 196, C4 29, Sed rate 35, ANA negative. The specimen is a renal biopsy.
Choose the Correct Diagnosis:
- Amyloid
- Immunotactoid glomerulopathy
- Cryoglobulinemic glomerulonephritis
- Fibrillary glomerulonephritis
The answer is “D,” Fibrillary glomerulonephritis
Fibrillary glomerulonephritis is an uncommon disease (about 1% of diagnoses among adults undergoing native kidney biopsy) of unknown etiology defined by deposition of fibrillary material in the glomerulus. It is a disease of adults (~50 years), involving most often Caucasian females. Most patients present with nephrotic syndrome and frequently have associated hematuria. Rapidly progressive glomerulonephritis can be seen in one third of patients. The prognosis is one of progression to renal loss in 40% of cases over 5 years. No specific treatment has been described.
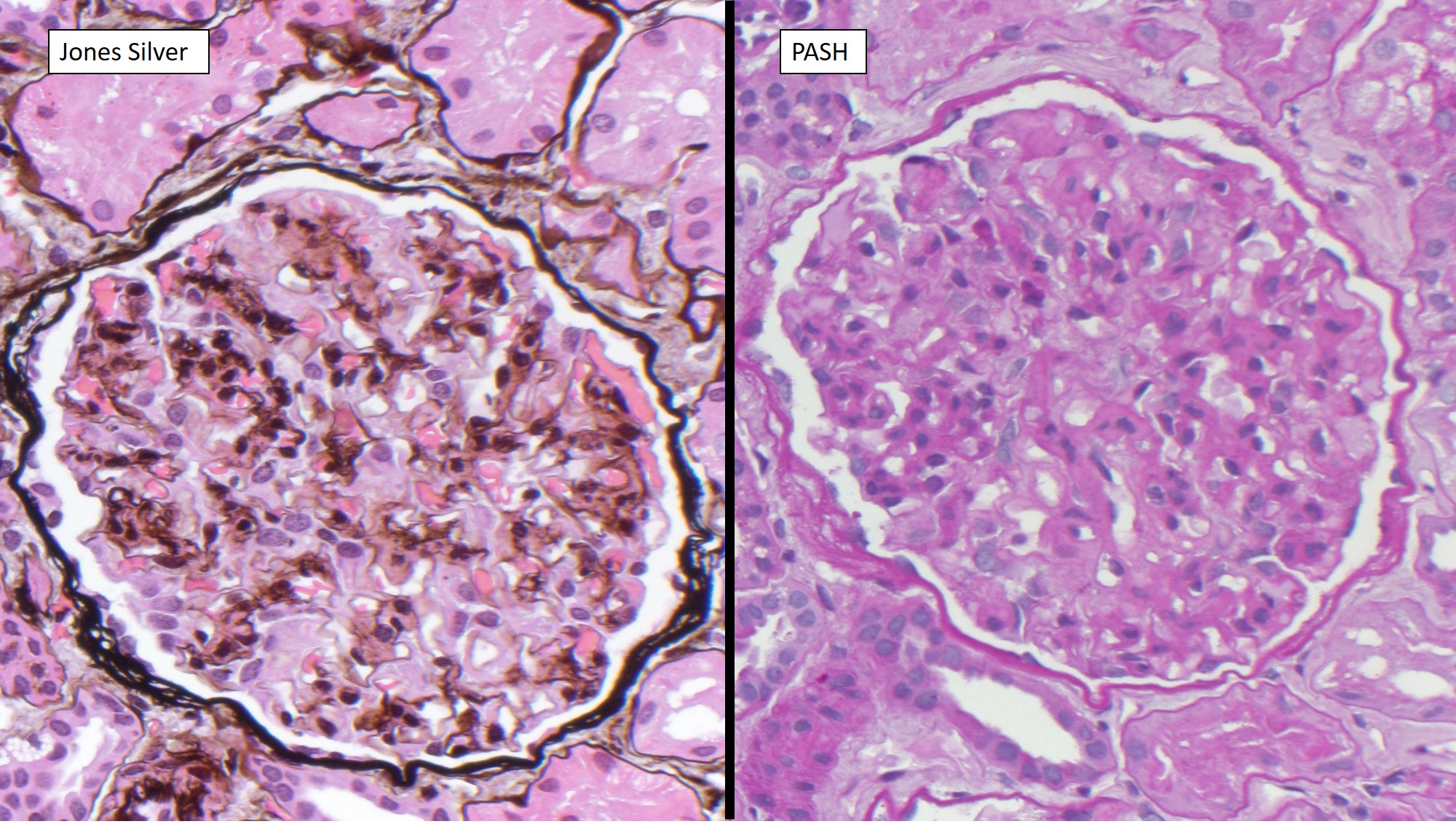
The light microscopic features include most frequently thickening of the glomerular capillary walls and expansion of the mesangial matrix by amorphous acellular material. The pattern of injury can be membranoproliferative, diffuse proliferative (with associated crescents) or mesangial proliferative; some cases may even appear similar to diabetic nephropathy. The areas of matrix expansion and deposits stain weakly PAS and silver positive and are Congo red negative.
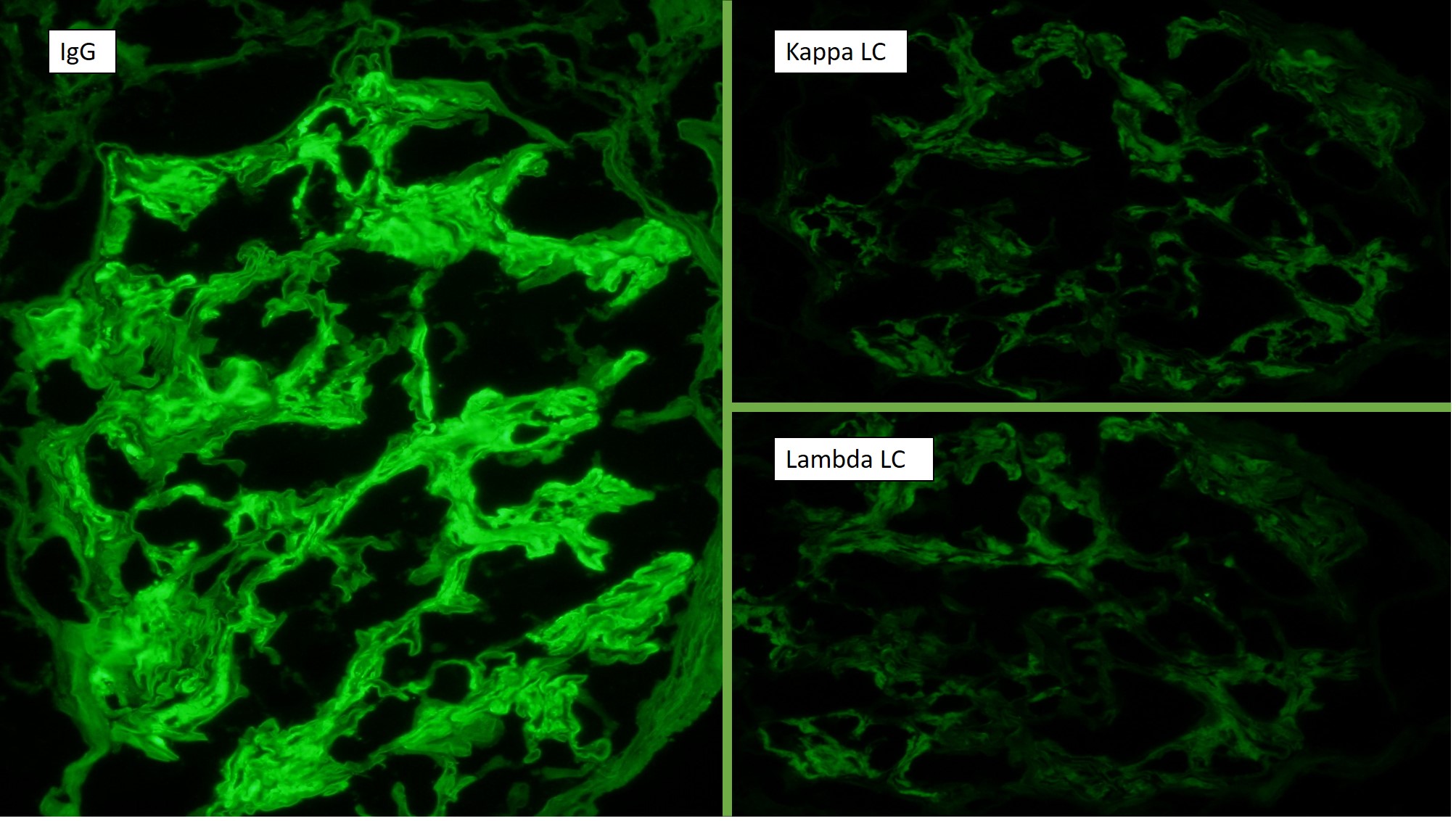
Immunofluorescence shows prominent, smudgy IgG and lesser amounts of C3 in mesangial areas, and segmental, usually chunky staining along GBM’s. In about half of cases, weaker IgA, IgM and C1q may also be detected.
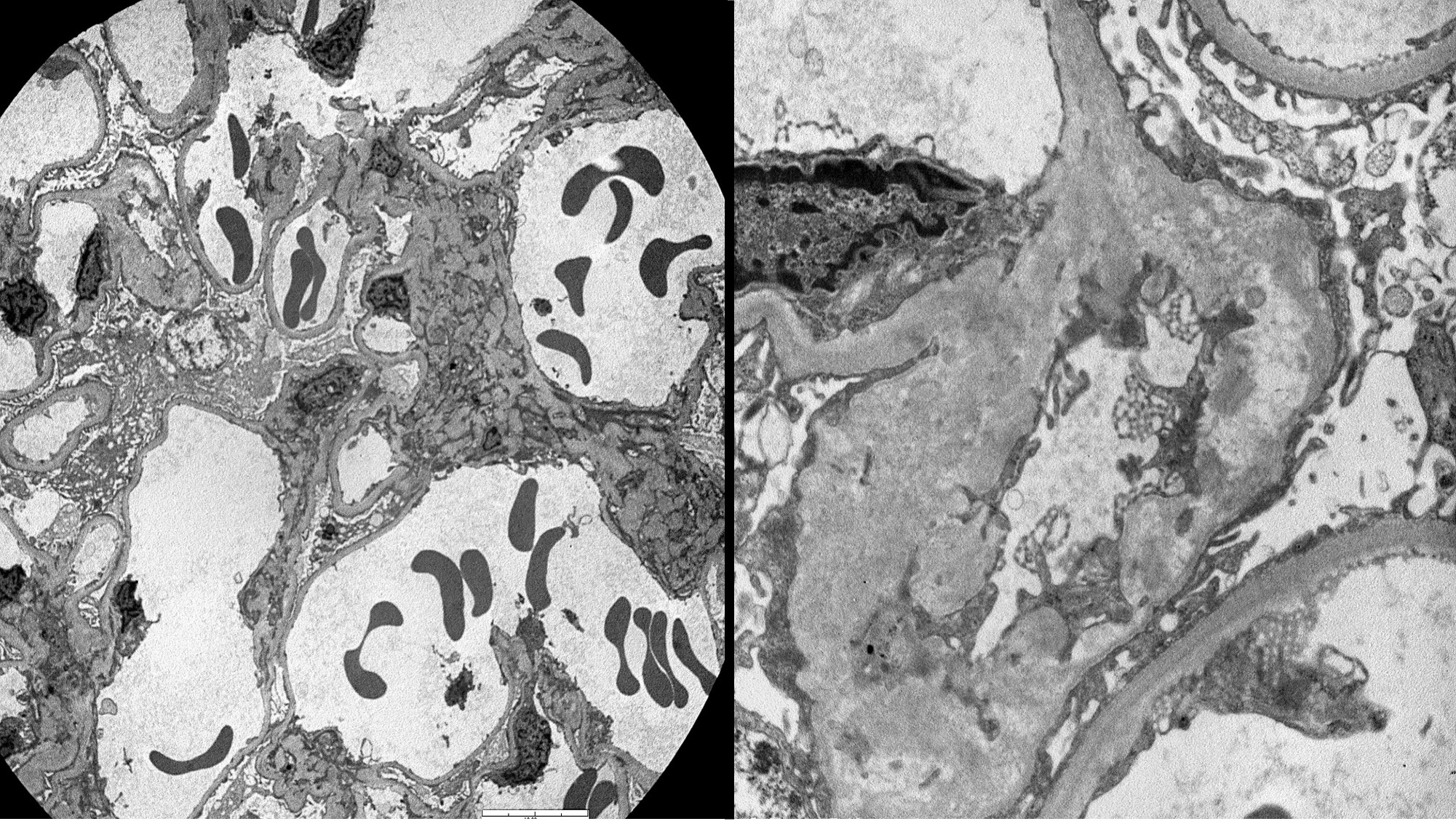
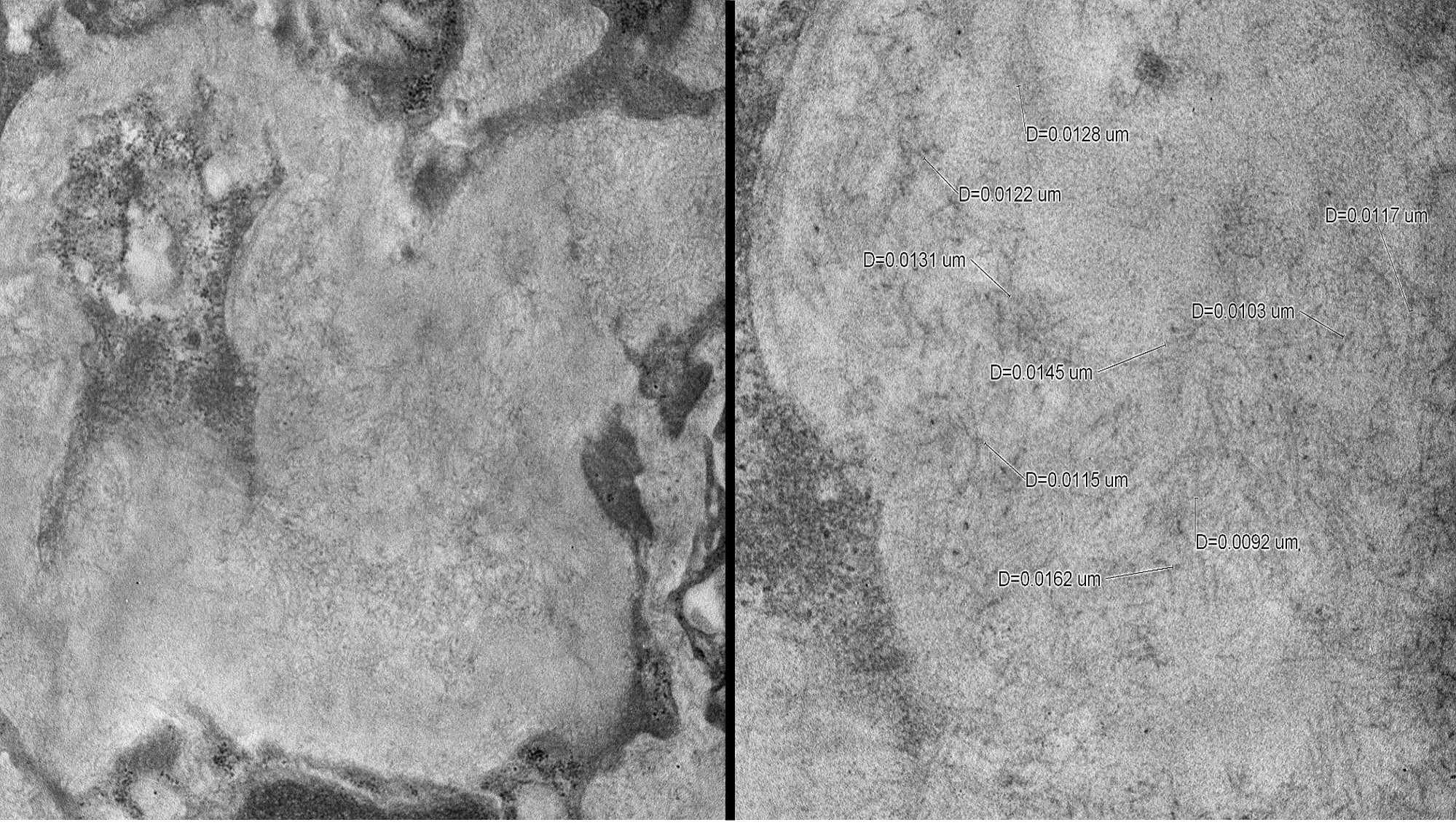
The electron microscopy findings show the presence of randomly aligned fibrils that resemble amyloid fibrils but are larger, with a range from 13-39nm (amyloid has a mean of 10nm). The fibrils can be present in all glomerular compartments, including mesangium and basement membranes.
Immunotactoid glomerulonephritis has a proliferative pattern on LM, IgG is often clonal, Congo red is negative, and the fibrils on EM are organized, parallel and microtubular with an average size greater than 30nm. Amyloid has an acellular, mesangial and lobular appearance on LM with monoclonal light chain for AL and positive Congo red; the fibrils are randomly arranged and measure mostly 10-12nm. Cryoglobulinemic glomerulonephritis has a proliferative morphology on LM with PAS-positive cryoplugs, often clonal IgM and negative Congo red; on EM, there is a microtubular configuration.
References
Fogo, Agnes B., and Michael Kashgarian. "1." Diagnostic Atlas of Renal Pathology. Philadelphia, PA: Elsevier, 2011. 94-101. Print.
Contributed by Frida Rosenblum, M.D., Assistant Professor, Anatomic Pathology, UAB Pathology